First Pass Techniques
What is the best technique for "first- pass" perfusion imaging?
|
|
Several methods are available for first-pass perfusion imaging but none has yet emerged as the unequivocal best choice. Any sequence selected for myocardial perfusion should ideally have the following characteristics:
|
Cine images from 1st pass myocardial perfusion study using a saturation recovery spoiled-GRE method
|
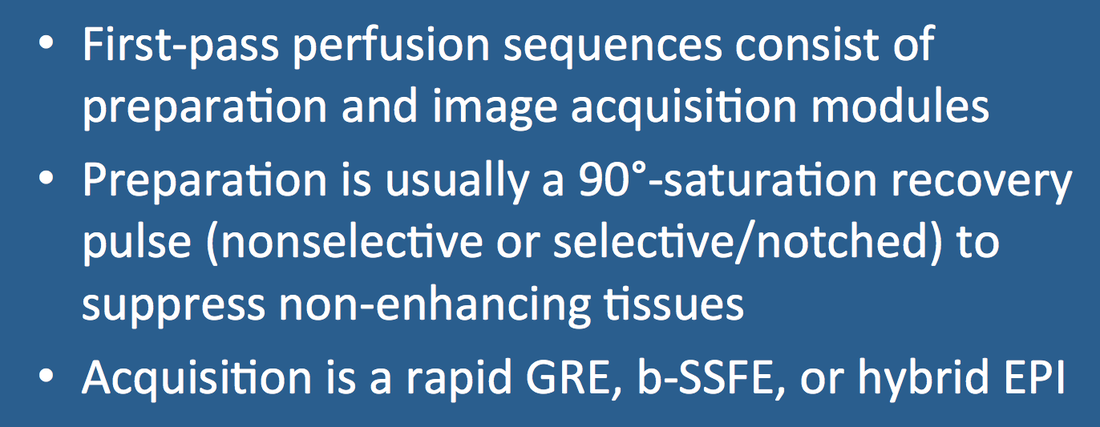
Sequences for first-pass perfusion consist of a magnetization preparation period followed by an image acquisition module. The purpose of the preparatory module is to reduce the signal of non-enhancing tissue so that gadolinium-enhancing blood and myocardium will be rendered more conspicuous. (This is analogous to background suppression commonly used in MR angiography to accentuate vessels).
Saturation recovery (SR) uses non-slice-selective 90º-pulses that tip the longitudinal magnetization (Mz) of all tissues in the imaging volume into the transverse plane. A crusher gradient (G) is typically applied immediately after the pulse to destroy transverse coherences. After being tipped into the transverse plane tissues begin to recover longitudinal magnetization as a function of their T1 values. Gadolinium-containing blood and myocardium have short T1's and recover quickly, while non-enhancing myocardium and other tissues remain relatively saturated/suppressed. An image acquisition module is then played out using a rapid sequence (spoiled-GRE, balanced-SSFP, or hybrid GRE-EPI). Lines at center of k-space are typically acquired at an "inversion" time (TI) of about 85 ms.
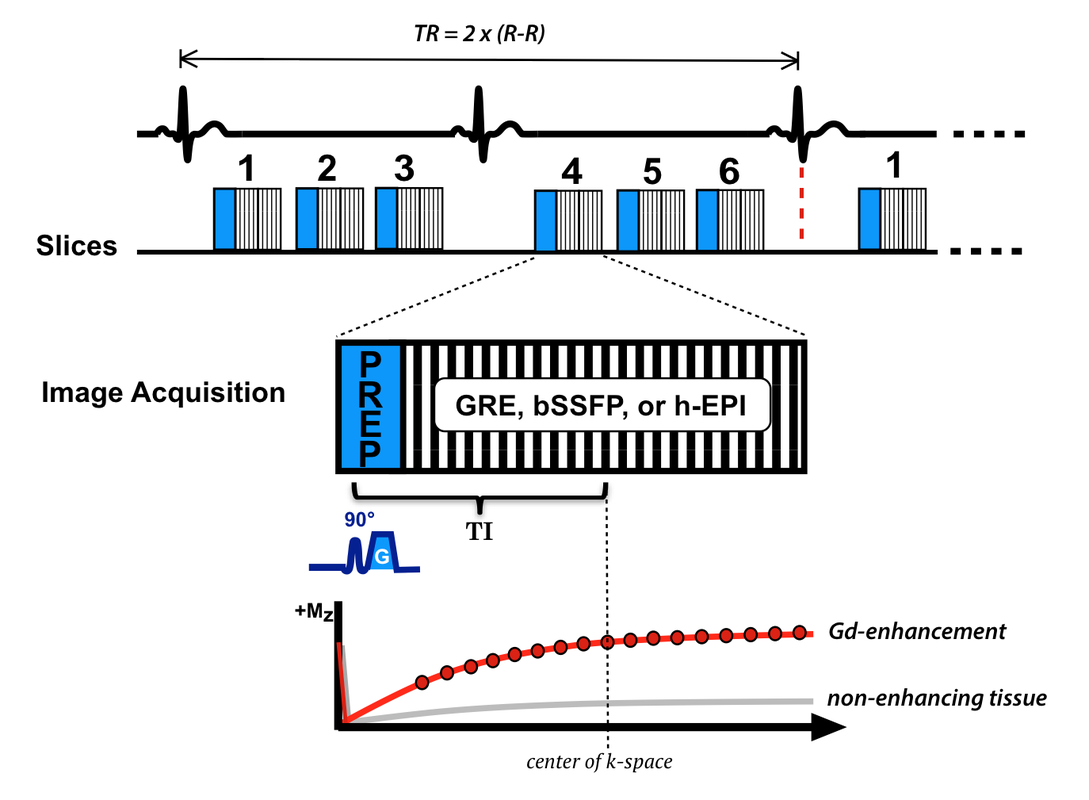
Saturation recovery (SR) myocardial perfusion sequence allowing for 3 slices every heartbeat (or 6 slices every two heartbeats). Here a 90º-nonselective pulse has been used to suppress signal from the entire volume before the image acquisition/readout by any of several methods. Between 64 and 128 lines of k-space are sampled for each slice with the center line at "inversion" time TI where an appreciable difference in signal is noted between enhancing and non-enhancing tissues.
Even better contrast between enhancing and non-enhancing tissues could be obtained by waiting a little longer between the saturation pulse and image acquisition (i.e., increasing TI). However, this would significantly lengthen imaging time per slice and reduce the maximum number of slices possible in a given R-R interval.
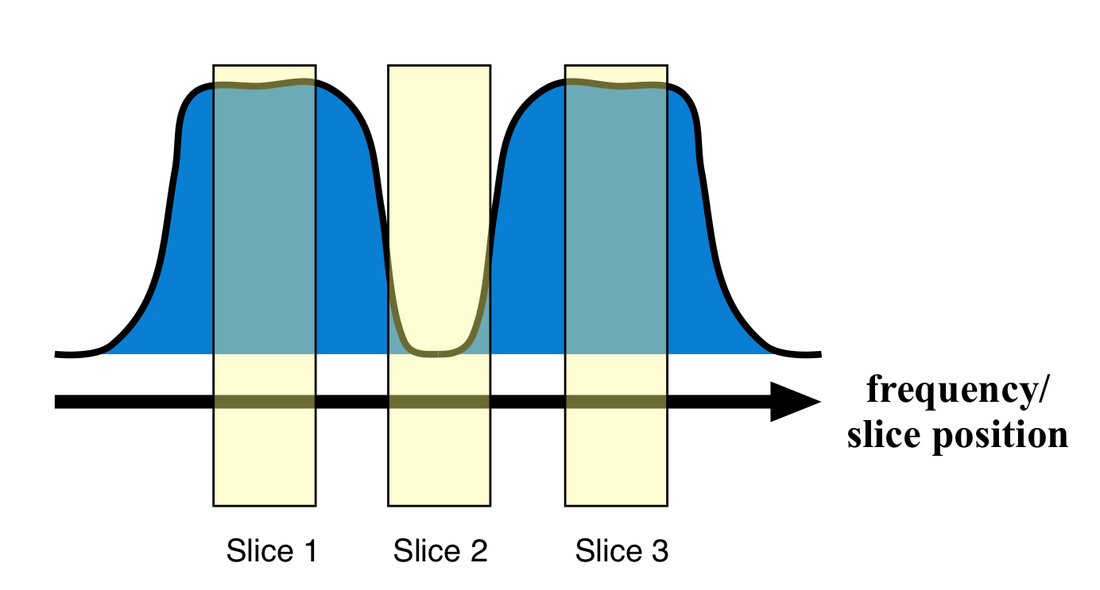
Slice profile of a "notched" RF-pulse. Slices 1 and 3 in the passband feel the brunt of the RF-pulse and are saturated, while Slice 2 (in the notch) is spared.
|
A clever method to permit lengthening of TI with little or no penalty in the number of slices is to use slice-selective notched RF-pulses. Notched RF-pulses saturate adjacent slices but have a mid-frequency gap leaving the center slice unaffected. TI is nearly doubled as the saturation pulse for a given slice has occurred when the previous slice was imaged. At present, this option is available only on GE scanners.
|
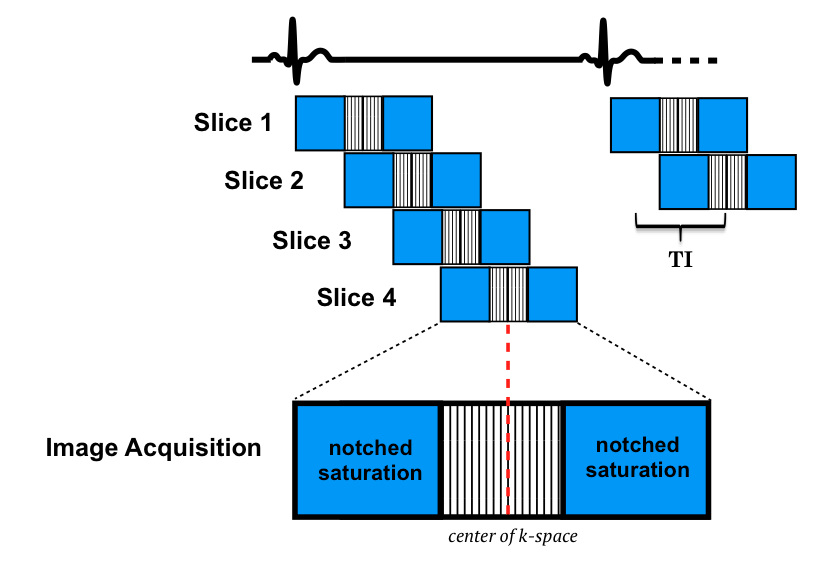
MR perfusion using notched saturation pulses (blue). Notched pulses contain a midfrequency gap while saturating adjacent slices. For example, the notched pulse corresponding to Slice 2 saturates Slices 1 and 3. This results in a longer inversion time (TI) with theoretically better image contrast.
Several other strategies and options for first-pass imaging exist but are not in widespread use. Interested readers should check the references and click the "Advanced Discussion" tab below.
References
Coelho-Filho OR, Rickers C, Kwong RY, Jerosch-Herold M. MR myocardial perfusion imaging. Radiology 2013; 266:701-725.
Ding S, Wolff SD, Epstein FH. Improved coverage in dynamic contrast-enhanced cardiac MRI using interleaved gradient-echo EPI. Magn Reson Med 1998; 39:514-519. (original description of hybrid EPI technique).
Fair MJ, Gatehouse PD, DiBella EVR, Firmin DN. A review of 3D first-pass, whole-heart, myocardial perfusion cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2015; 17:68e
Gerber BL, Raman SV, Nayak K, et al. Myocardial first-pass perfusion cardiovascular magnetic resonance: history, theory and current state of the art. J Cardiovasc Magn Reson 2008; 10:18.
Hunold P, Maderwald S, Eggebrecht, et al. Steady-state free precession sequences in myocardial first-pass perfusion MR imaging: comparison with TurboFLASH imaging. Eur Radiol 2004; 14:409-416
Jung B, Honal M, Hennig J, Markl M. k-t-Space accelerated myocardial perfusion. J Magn Reson Imaging 2008; 28:1080-1085.
Kellman P, Arai AE. Imaging sequences for first pass perfusion − a review. J Cardiovasc Magn Reson 2007; 9:525-537.
Shehata ML, Basha T, Hayeri MR, et al. MR myocardial perfusion imaging: insights on techniques, analysis, interpretation, and findings. RadioGraphics 2014; 32:1636-1657.
Slavin GS, Wolff SD, Gupta SN, Foo TKF. First-pass myocardial perfusion MR imaging with interleaved notched saturation: feasibility study. Radiology 2001; 219:258-163. (The notched RF method).
Wang Y, Moin K, Akinboboye O, Reichek N. Myocardial first pass perfusion: steady-state free precession versus spoiled gradient echo and segmented echo planar imaging. Magn Reson Med 2005; 54:1123-1129.
Coelho-Filho OR, Rickers C, Kwong RY, Jerosch-Herold M. MR myocardial perfusion imaging. Radiology 2013; 266:701-725.
Ding S, Wolff SD, Epstein FH. Improved coverage in dynamic contrast-enhanced cardiac MRI using interleaved gradient-echo EPI. Magn Reson Med 1998; 39:514-519. (original description of hybrid EPI technique).
Fair MJ, Gatehouse PD, DiBella EVR, Firmin DN. A review of 3D first-pass, whole-heart, myocardial perfusion cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2015; 17:68e
Gerber BL, Raman SV, Nayak K, et al. Myocardial first-pass perfusion cardiovascular magnetic resonance: history, theory and current state of the art. J Cardiovasc Magn Reson 2008; 10:18.
Hunold P, Maderwald S, Eggebrecht, et al. Steady-state free precession sequences in myocardial first-pass perfusion MR imaging: comparison with TurboFLASH imaging. Eur Radiol 2004; 14:409-416
Jung B, Honal M, Hennig J, Markl M. k-t-Space accelerated myocardial perfusion. J Magn Reson Imaging 2008; 28:1080-1085.
Kellman P, Arai AE. Imaging sequences for first pass perfusion − a review. J Cardiovasc Magn Reson 2007; 9:525-537.
Shehata ML, Basha T, Hayeri MR, et al. MR myocardial perfusion imaging: insights on techniques, analysis, interpretation, and findings. RadioGraphics 2014; 32:1636-1657.
Slavin GS, Wolff SD, Gupta SN, Foo TKF. First-pass myocardial perfusion MR imaging with interleaved notched saturation: feasibility study. Radiology 2001; 219:258-163. (The notched RF method).
Wang Y, Moin K, Akinboboye O, Reichek N. Myocardial first pass perfusion: steady-state free precession versus spoiled gradient echo and segmented echo planar imaging. Magn Reson Med 2005; 54:1123-1129.