Orbital Foreign Bodies
I've heard people have been blinded by metallic foreign bodies in the eye. How do you screen for these?
|
|
Sentinel Case (reported in AJNR 1986)
Sentinel Case (California, 1985): A former sheet-metal worker was blinded from motion of an occult 2.0 x 3.5 mm intra-ocular metallic fragment during MR imaging at 0.35 T. Although the fragment had been seen on CT as well as on ophthalmologic examination, it was misdiagnosed as a post-inflammatory calcification, likely an old parasitic (Toxicara) granuloma. As the table was being moved out at the end of the completed MRI exam, the patient experienced a tugging sensation in his eye, a flash of light, then a dramatic decrease in vision. Examination revealed massive vitreous hemorrhage and retinal laceration.
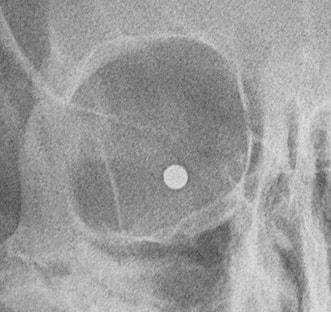
Patient with a BB in the orbit. No MRI for you!
|
This justifiably infamous case shocked all of us working in the early days of clinical MRI. It stimulated everyone to adopt more rigorous standards for screening patients for orbital metallic foreign bodies. Either as a result of improved screening, or more likely in spite of it, there have been no cases of blindness and only four (4) additional reported metallic foreign body eye-related MR incidents since 1985 (details of each are summarized in the References below). This is against a background of over 500 million MRI scans being performed worldwide during the same period.
|
Two of these reports described transient hyphemas (bleeding in the anterior chamber) that were cleared or resolving without treatment; one case described local eye pain (possibly heating related) that resolved immediately after removal from the scanner; the fourth report is of a patient had no immediate signs/symptoms, but later developed a cataract (which seems likely to have been the result of his initial injury, not the MRI).
Because the risk of significant eye injury is extraordinarily low, we successfully adopted the strategy (based on the cost-effectiveness model of Seidenwurm) and used it without incident in over 500,000 cases during my tenure at Wake Forest. We ask the following during screening:
|
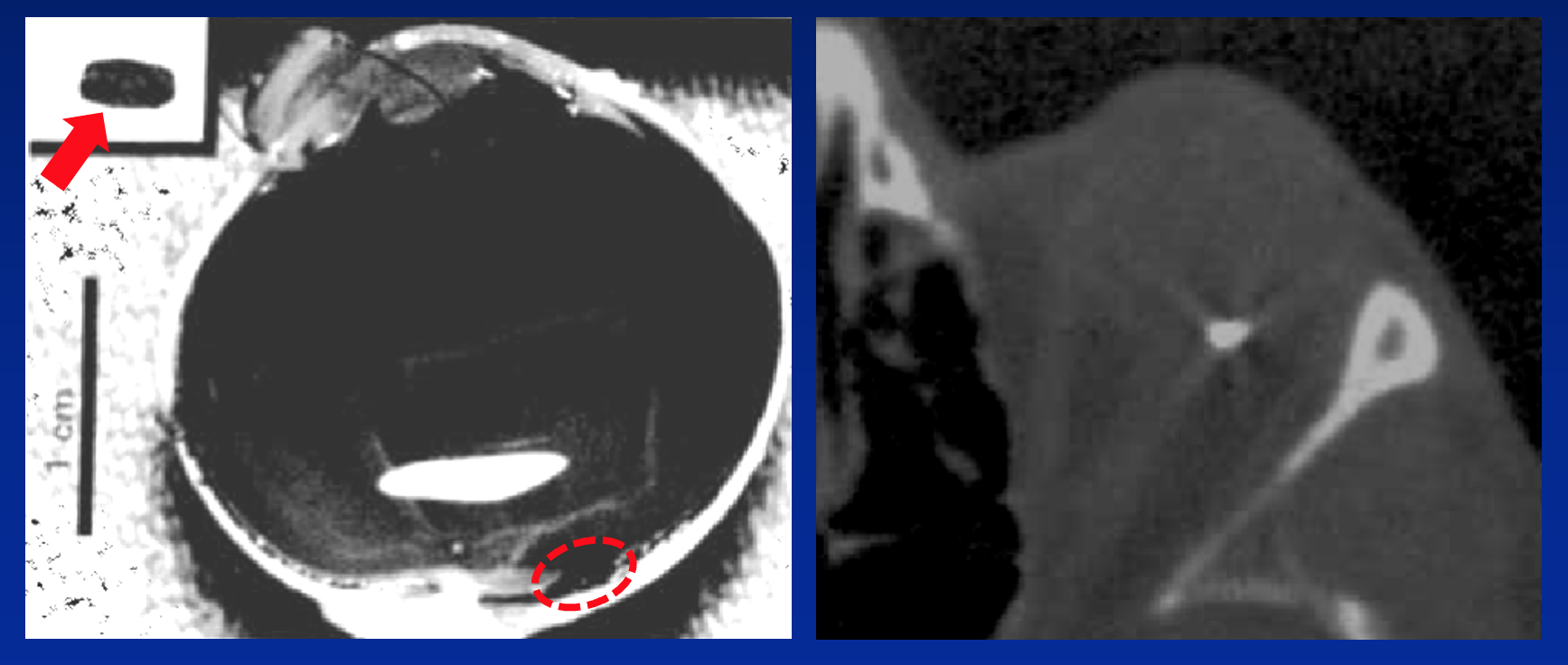
In brief, we believe that mere occupational exposure to metal fragments is not sufficient to warrant additional radiographic workup. If there is reasonable suspicion that an orbital metal fragment is present, or if the patient seems unsure, then we investigate further, first reviewing any head CT, MR, or radiology studies obtained after the injury. It these do not exist or cannot easily be located, we then proceed with plain films of the orbits for screening.
Although some have advocated the use of orbital CT for this purpose, experimental evidence in cadavers has shown that the threshold size of metallic particle detection using CT (~0.4 mm) is not remarkably superior to that of plain films (~0.5 mm). Furthermore, it is unlikely that particles ≤ 0.5 mm in size from industrial sources will penetrate the sclera or cause significant injury from MRI if they do.
References
Chaco JG, Figueroa RE, Johnson MH, et al. Detection and localization of steel intraocular foreign bodies using computed tomography. A comparison of helical and conventional axial scanning. Ophthalmology 1997; 104:319-323. [DOI LINK] (1-mm helical CT detects 100% of orbital metallic FB's of size ≥ 0.06 mm³, or ~0.4 mm diameter)
Jarvik JG, Ramsey S. Radiographic screening for orbital foreign bodies prior to MR imaging: is it worth it? AJNR Am J Neuroradiol. 2000; 21:245–247 (editorial on the Seidenwurm article, largely supporting its conclusions).
Kelly WM, Paglen PG, Pearson JA, et al. Ferromagnetism of intraocular foreign body causes unilateral blindness after MR study. AJNR Am J Neuroradiol 1986; 7:243-6. (the Sentinel Case abstracted above)
Lawrence DA, Lipman AT, Gupta SK, Lacey NC. Undetected intraocular metallic foreign body causing hyphema in a patient undergoing MRI: a rare occurrence demonstrating the limitations of pre-MRI safety screening. Magn Reson Imaging 2015; 33:358-361. [DOI Link] (a relatively minor complication from 1-2 mm FB — a small amount of blood localized to anterior chamber, causing delayed blurred vision that resolved completely in 2 weeks)
Maralani PJ, Schieda N, Hecht EM, et al. MRI safety and devices: an update and expert consensus. J Magn Reson Imaging 2019; 51:657-674. [DOI LINK]
Mamas N, Andreanos K, Brouzas D, et al. Acute ocular pain during magnetic resonance imaging due to retained intraocular metallic foreign body: the role of ultrasonography and ultrasound biomicroscopy in diagnosis and management of this condition. J Ultrasound 2018; 21:159-163. [DOI LINK] (2-3 mm FB in pars plana of ciliary body; patient experienced acute eye pain during MR exam that resolved completely when removed from scanner; my take -- probable heating of tissues near metal rather than movement).
Otto PM, Otto RA, Virapongse C, et al. Screening test for detection of metallic foreign objects in the orbit before magnetic resonance imaging. Invest Radiol 1992; 27:308-11. [DOI LINK] (orbit x-rays reliably detect metallic FBs of size ≥ 0.12 mm³, or ~0.5 mm diameter)
Seidenwurm DJ, McDonnell III CH, Raghavan N, Breslau J. Cost utility analysis of radiographic screening for an orbital foreign body before MR imaging. AJNR Am J Neuroradiol. 2000; 21:426–433. [DOI LINK]. (excellent paper that in my opinion, set a reasonable, cost-effective approach to ocular FB screening that we used at Wake Forest for 10+ years without incident).
Ta CN, Bowman RW. Hyphema caused by a metallic intraocular foreign body during magnetic resonance imaging. Am J Ophthalmol 2000; 129:533–4. [DOI Link] (approx. 1-mm FB in inferior anterior chamber created pain and vision loss with 50% hyphema; hyphema largely resolved with improving vision, but patient died of unrelated causes 5 days later).
Vote BJ, Simpson AJ. X-ray turns a blind eye to ferrous metal. Clin Experiment Ophthalmol 2001;29:262–4. [DOI Link] (~0.7-mm fragment in anterior chamber near inferior iris was present on screening x-rays but overlooked; no acute damage to eye; patient did develop a post-traumatic cataract over the next several months, but this seems likely to have resulted from his initial accident when he acquired the FB, not MRI-related movement of the FB itself.)
Zhang Y, Cheng J, Bai J, et al. Tiny ferromagnetic intraocular foreign bodies detected by magnetic resonance imaging: A report of two cases. J Magn Reson Imaging 2009; 29:704–707. [DOI Link] (2 cases of orbital FB's smaller than 0.5 mm scanned at 1.0T without complications)
Chaco JG, Figueroa RE, Johnson MH, et al. Detection and localization of steel intraocular foreign bodies using computed tomography. A comparison of helical and conventional axial scanning. Ophthalmology 1997; 104:319-323. [DOI LINK] (1-mm helical CT detects 100% of orbital metallic FB's of size ≥ 0.06 mm³, or ~0.4 mm diameter)
Jarvik JG, Ramsey S. Radiographic screening for orbital foreign bodies prior to MR imaging: is it worth it? AJNR Am J Neuroradiol. 2000; 21:245–247 (editorial on the Seidenwurm article, largely supporting its conclusions).
Kelly WM, Paglen PG, Pearson JA, et al. Ferromagnetism of intraocular foreign body causes unilateral blindness after MR study. AJNR Am J Neuroradiol 1986; 7:243-6. (the Sentinel Case abstracted above)
Lawrence DA, Lipman AT, Gupta SK, Lacey NC. Undetected intraocular metallic foreign body causing hyphema in a patient undergoing MRI: a rare occurrence demonstrating the limitations of pre-MRI safety screening. Magn Reson Imaging 2015; 33:358-361. [DOI Link] (a relatively minor complication from 1-2 mm FB — a small amount of blood localized to anterior chamber, causing delayed blurred vision that resolved completely in 2 weeks)
Maralani PJ, Schieda N, Hecht EM, et al. MRI safety and devices: an update and expert consensus. J Magn Reson Imaging 2019; 51:657-674. [DOI LINK]
Mamas N, Andreanos K, Brouzas D, et al. Acute ocular pain during magnetic resonance imaging due to retained intraocular metallic foreign body: the role of ultrasonography and ultrasound biomicroscopy in diagnosis and management of this condition. J Ultrasound 2018; 21:159-163. [DOI LINK] (2-3 mm FB in pars plana of ciliary body; patient experienced acute eye pain during MR exam that resolved completely when removed from scanner; my take -- probable heating of tissues near metal rather than movement).
Otto PM, Otto RA, Virapongse C, et al. Screening test for detection of metallic foreign objects in the orbit before magnetic resonance imaging. Invest Radiol 1992; 27:308-11. [DOI LINK] (orbit x-rays reliably detect metallic FBs of size ≥ 0.12 mm³, or ~0.5 mm diameter)
Seidenwurm DJ, McDonnell III CH, Raghavan N, Breslau J. Cost utility analysis of radiographic screening for an orbital foreign body before MR imaging. AJNR Am J Neuroradiol. 2000; 21:426–433. [DOI LINK]. (excellent paper that in my opinion, set a reasonable, cost-effective approach to ocular FB screening that we used at Wake Forest for 10+ years without incident).
Ta CN, Bowman RW. Hyphema caused by a metallic intraocular foreign body during magnetic resonance imaging. Am J Ophthalmol 2000; 129:533–4. [DOI Link] (approx. 1-mm FB in inferior anterior chamber created pain and vision loss with 50% hyphema; hyphema largely resolved with improving vision, but patient died of unrelated causes 5 days later).
Vote BJ, Simpson AJ. X-ray turns a blind eye to ferrous metal. Clin Experiment Ophthalmol 2001;29:262–4. [DOI Link] (~0.7-mm fragment in anterior chamber near inferior iris was present on screening x-rays but overlooked; no acute damage to eye; patient did develop a post-traumatic cataract over the next several months, but this seems likely to have resulted from his initial accident when he acquired the FB, not MRI-related movement of the FB itself.)
Zhang Y, Cheng J, Bai J, et al. Tiny ferromagnetic intraocular foreign bodies detected by magnetic resonance imaging: A report of two cases. J Magn Reson Imaging 2009; 29:704–707. [DOI Link] (2 cases of orbital FB's smaller than 0.5 mm scanned at 1.0T without complications)
Related Questions
How do you screen patients for implants and foreign bodies prior to MRI?
Which types of metal are the most dangerous around a magnetic field?
How do you screen patients for implants and foreign bodies prior to MRI?
Which types of metal are the most dangerous around a magnetic field?