Flow Appearance on MRIHow can you predict whether a certain vessel will be bright or dark on an MR image?
|
|
Experienced radiologists generally become familiar with the expected appearances of normal blood vessels on their own scanners when consistent imaging parameters are used; and at times they may even be capable of diagnosing subtle disorders of flow by using pattern recognition. However, no radiologist, even a world "expert", can consistently predict (or even fully explain) the complex signals observed within any vessel, given an arbitrary set of imaging parameters. The reason for this uncertainty is that the appearance of flowing blood on MR images depends in a complex and nonintuitive fashion both on the details of the pulse sequence employed and the physical characteristics of flow.
Technical factors affecting the appearance of flowing blood include the type of pulse sequence (spin echo, gradient echo, inversion recovery), repetition time (TR), echo time (TE), and flip angle (α). The use of flow compensation (gradient-moment nulling), saturation pulses, and cardiac gating also has profound effects. Additionally, even small changes in slice thickness, interslice gap, number of slices, or slice excitation order may have radical effects on the appearance of normal blood vessels at MR imaging. Marked variations in the appearance of flow may also exist between different brands of scanners run with otherwise identical user-specified parameters.
Physical characteristics of flow are also important determinants of a vessel's appearance on MR images. These characteristics include not only flow direction and average velocity, but also acceleration, pulsatility, and the distribution of velocities across the vessel. The internal "structure" of the flow is important, as differences are noted between laminar, vortex, and turbulent patterns. No wonder even sophisticated computer programs are not yet fully able to predict the wide spectrum of normal vascular appearances encountered on MR images!
Notwithstanding these uncertainties, several general principles can be derived concerning the appearance of flow on MR images:
- Rapid or turbulently flowing fluids generally have low signal on conventional spin-echo images, resulting in a so-called flow void.
- Conversely, slowly flowing blood or CSF generally appears bright on conventional spin-echo images, a phenomenon sometimes called paradoxical enhancement.
- Fresh blood flowing into a volume of tissue results in high intravascular signal at the end slices of a multisection acquisition; this is a time-of-flight effect called flow-related enhancement or simply the entry phenomenon.
- Saturation pulses applied outside the field of view will reduce or eliminate the entry phenomenon, making these vessels dark.
- The use of gradient-moment nulling (flow compensation) gradients will result in increased signal within veins and smaller arteries, but faster flow in larger arteries will still demonstrate flow voids.
- Cardiac gating may restore signal not only to small vessels, but to larger ones as well.
- Two different flow-related signal changes may be observed when trains of evenly spaced (i.e., TE=30/60/90/120) spin echoes are employed. Loss of signal occurs after odd-numbered (i.e., 30, 90) echoes (odd-echo dephasing) whereas increased signal will be seen on even-numbered (60, 120) echoes (even-echo rephasing).
- Gadolinium contrast shortens the T1 of blood and generally increases the signal from all vessels, but especially veins.
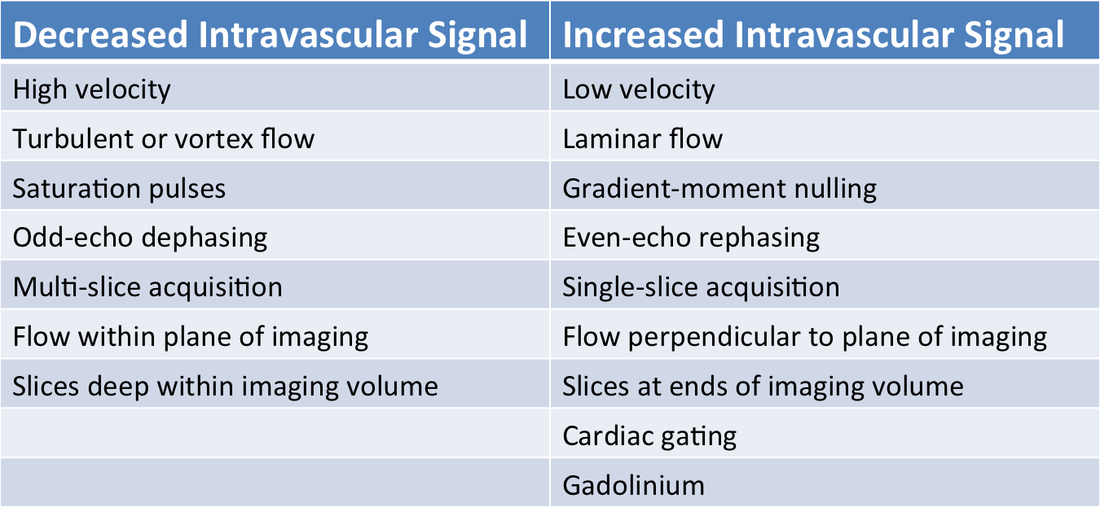
These concepts are summarized in the table below and will be further explained in other Q&A's within this tab.
Factors Affecting the MR Signal Observed in Blood Vessels
References
Axel L. Blood flow effects in magnetic resonance imaging. AJR Am J Roentgenol 1984; 143:1157-1166.
Urchuk SN, Plewes DB. Mechanisms of flow‑induced signal loss in MR angiography. J Magn Reson Imaging 1992; 2:453-462.
Axel L. Blood flow effects in magnetic resonance imaging. AJR Am J Roentgenol 1984; 143:1157-1166.
Urchuk SN, Plewes DB. Mechanisms of flow‑induced signal loss in MR angiography. J Magn Reson Imaging 1992; 2:453-462.