Bowel Contrast Agents
Do you use bowel contrast agents for abdominal MR imaging?
|
|
For routine abdominal imaging, we seldom use any type of enteric contrast agent. However, we regularly use orally administered contrast when intrinsic diseases of the bowel wall or mesentery are evaluated, as for MR enterography. The goal of all such agents is to distend collapsed loops of bowel while replacing ingested food and air by a material with a uniform consistency.
Enteric MR contrast materials are often classified by their effects on the signal of bowel contents. Biphasic contrast agents lengthen both T1 and T2 values, resulting in decreased intraluminal signal on T1 weighted images and increased signal on T2-weighted images. Water is the simplest example of a biphasic agent. Positive contrast agents shorten T1 relaxation times and increase intraluminal signal on T1-weighted images. Negative contrast agents shorten T2 relaxation times and decrease intraluminal signal on T2-weighted images. Positive and negative contrast agents typically utilize paramagnetic or diamagnetic materials to create these effects.
Biphasic contrast agents are all water-based, appearing dark on T1-weighted and bright on T2-weighted images. Although in large quantities pure water provides good distention of the stomach and duodenum, it is resorbed rapidly in the jejunum making it an inadequate contrast agent for most small bowel imaging.
To overcome this limitation, biphasic enteric contrast agents contain nonabsorbable additives (resins, polyethylene glycol, mannitol, sorbitol, or other sugar alcohols) that help draw in and retain intraluminal water. Although many "make your own" recipes are available, we prefer to use a commercially available product (NeuLumEX®, formerly VoLumen®, Bracco Diagnostics, Princeton, NJ), already approved and widely used for CT enterography. A similar product (Breeza Beekley Medical, Bristol, CT) is a well-tolerated alternative, being marketed as a “flavored beverage.”
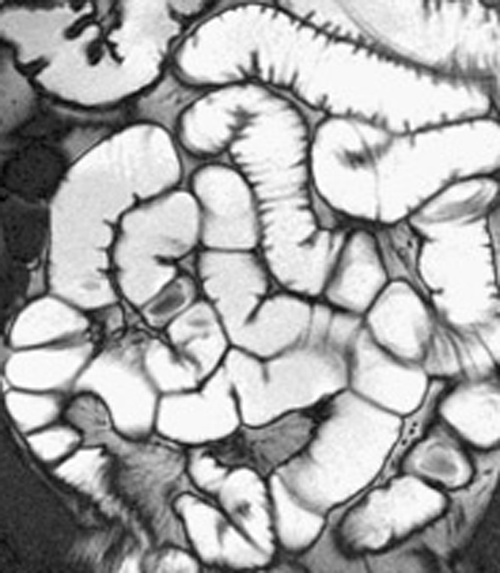 MR enterography with VoLumen
MR enterography with VoLumen
NeuLumEX® is a thin (0.1% w/v) barium sulfate solution with a blueberry flavoring. It contains 1.4% sorbitol as well as gum resins and barium that contribute to water retention by its hyperosmolar nature. These benefits for imaging also create problems for the patient; many complain of severe abdominal cramping, nausea, vomiting, and diarrhea after consuming this material.
Before imaging, patients are asked to drink approximately 1 L of VoLumen over a 30-45 minute period. They may also be given 10 mg of metoclopramide (to promote gastric emptying) and 0.5 mg of glucagon IV (to reduce peristalsis). Increased water within the bowel means that the intraluminal contents will have long T1 and T2 values. In MR enterography T2-weighted ultrafast breath-hold sequences like HASTE or TrueFISP are are typically used rendering the intestinal contents bright and their walls dark.
Before imaging, patients are asked to drink approximately 1 L of VoLumen over a 30-45 minute period. They may also be given 10 mg of metoclopramide (to promote gastric emptying) and 0.5 mg of glucagon IV (to reduce peristalsis). Increased water within the bowel means that the intraluminal contents will have long T1 and T2 values. In MR enterography T2-weighted ultrafast breath-hold sequences like HASTE or TrueFISP are are typically used rendering the intestinal contents bright and their walls dark.
Positive contrast agents shorten relaxation times and increase intraluminal signal on T1-weighted images. This is usually accomplished using low concentrations of ferric, manganese, or gadolinium ions. In the 1990's several of these agents were commercially available, including an enteral formulation of Magnevist® (Gd-DTPA) and LumenHance® (MnCl2). Neither agent is still in production. Some researchers have recommended the use of blueberry or pineapple juice as positive contrast agents, since both contain naturally high levels of manganese. In a different strategy, orally administered lipids with short T1 values (e.g., mineral oils, emulsions, and sucrose polyesters) have also been evaluated as positive contrast agents.
Negative contrast agents are designed to make the intraluminal contents dark, especially on T2-weighted images. This can be done by filling the bowel with diamagnetic materials (barium, kaolin) or relatively high concentrations of paramagnetic ions (where very short T2 values dominate the effects of short T1s). The use of perfluorochemicals (molecules where H atoms are replaced by F atoms) at one time seemed promising, giving rise to a now discontinued product (Imagent GI®). At present the most popular negative enteric agents use superparamagnetic ion oxides (SPIOs) to produce marked T2* shortening.
|
GastroMARK® (ferumoxsil) is such a product — an oral suspension of siloxane-coated magnetite nanoparticles. GastroMARK® causes a remarkable drop in signal within the bowel lumen on both T1 and T2-weighted images. The darkening on T1-weighted images allows visualization of mucosal enhancement. Some centers mix NeuLumEX® and GastroMARK® as a combined agent. Like VoLumen®, GastroMARK® also causes abdominal pain and diarrhea in up to 30% of patients. And, as a bonus, it tastes terrible!
|
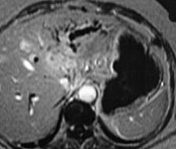
Negative bowel contrast agent (GastroMARK) in the stomach.
|
References
ACR Committee on Drugs and Contrast Agents. ACR Manual on Contrast Agents, 2024. American College of Radiology, 2024.
Chatterji M, Fidler JL, Taylor SA, et al. State of the art MR enterography technique. Top Magn Res Imaging 2021; 30:3-11. [DOI LINK]
Gee MS, Harisinghani MG. MRI in patients with inflammatory bowel disease. J Magn Reson Imaging 2011; 33:527-534.
Kuehle CA, Ajaj W, Ladd SC, et al. Hydro-MRI of the small bowel: effect of contrast volume, timing of contrast administration, and data acquisition on bowel distension. AJR Am J Roentgenol 2006; 187:W375-385.
Mallinkrodt Inc. GastroMARK® package insert/prescribing information. Accessed 1/1/15.
Papanikolauou N, Karantanas A, Maris T, Gourtsoyiannis N. MR cholangiopancreatography before and after oral blueberry juice administration. J Comput Assist Tomogr 2000; 24:229-234.
Rinck PA, Smevik O, Nilsen G, et al. Oral magnetic particles in MR imaging of the abdomen and pelvis. Radiology 1991;178:775.
ACR Committee on Drugs and Contrast Agents. ACR Manual on Contrast Agents, 2024. American College of Radiology, 2024.
Chatterji M, Fidler JL, Taylor SA, et al. State of the art MR enterography technique. Top Magn Res Imaging 2021; 30:3-11. [DOI LINK]
Gee MS, Harisinghani MG. MRI in patients with inflammatory bowel disease. J Magn Reson Imaging 2011; 33:527-534.
Kuehle CA, Ajaj W, Ladd SC, et al. Hydro-MRI of the small bowel: effect of contrast volume, timing of contrast administration, and data acquisition on bowel distension. AJR Am J Roentgenol 2006; 187:W375-385.
Mallinkrodt Inc. GastroMARK® package insert/prescribing information. Accessed 1/1/15.
Papanikolauou N, Karantanas A, Maris T, Gourtsoyiannis N. MR cholangiopancreatography before and after oral blueberry juice administration. J Comput Assist Tomogr 2000; 24:229-234.
Rinck PA, Smevik O, Nilsen G, et al. Oral magnetic particles in MR imaging of the abdomen and pelvis. Radiology 1991;178:775.
Related Questions
Whatever happened to Feridex®? Aren't iron-containing contrast agents useful for liver MRI?
Whatever happened to Feridex®? Aren't iron-containing contrast agents useful for liver MRI?