Vagal Nerve Stimulators
Can vagal nerve stimulators be safely scanned? |
|
Vagal Nerve Stimulators for Neurologic Disease
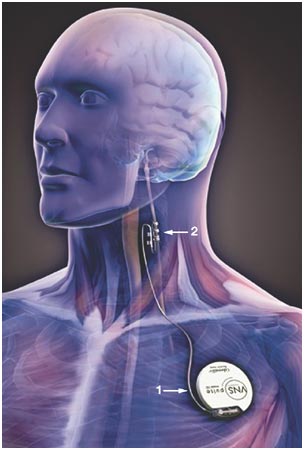 LivaNova VNS Therapy® System
LivaNova VNS Therapy® System
The most common neurologic applications for Vagal Nerve Stimulator (VNS) systems include drug-refractory epilepsy and depression. A single company (LivaNova, formerly Cyberonics) produces virtually all VNS systems for neurologic use world-wide. Current models include the AspireSR® and Sentiva™.
VNS systems resemble cardiac pacemakers. They consist of a battery and pulse generator (typically implanted subcutaneously in the upper chest) and a lead with terminal electrodes placed adjacent to a segment of the vagus nerve (usually in the mid-neck).
The standard stimulation regimen is 30 seconds every 5 minutes, but can be adjusted by an external programming device on a patient-by-patient basis. Newer models also detect changes in heart rate (that can increase immediately before a seizure) and automatically apply extra stimulating pulses. An external hand-held magnet placed over the pulse generator can temporarily increase stimulation rate when needed during a seizure
VNS systems resemble cardiac pacemakers. They consist of a battery and pulse generator (typically implanted subcutaneously in the upper chest) and a lead with terminal electrodes placed adjacent to a segment of the vagus nerve (usually in the mid-neck).
The standard stimulation regimen is 30 seconds every 5 minutes, but can be adjusted by an external programming device on a patient-by-patient basis. Newer models also detect changes in heart rate (that can increase immediately before a seizure) and automatically apply extra stimulating pulses. An external hand-held magnet placed over the pulse generator can temporarily increase stimulation rate when needed during a seizure
LivaNova VNS Therapy® devices are classified as MR Conditional. Device interrogation and programming is required by a healthcare professional both before and after MR imaging. Prior to entering the MR system room settings from the device should be recorded and output current set to zero. Standard limitations (field strength, SAR, etc) must be strictly followed. Very strict limitations concerning RF-exposure vary by the model and location of the pulse generator. In general use of transmit-receive head or extremity coils are preferred, and use of a transmit body coil for imaging the C7-L3 area is not permitted. (But see Advanced Discussion for further comments on exclusion zones). As an additional warning, patients with VNS systems often carry with them small clip-on magnets used to turn their devices on and off. These could potentially become dangerous projectiles if inadvertently carried into the MR scanning room.
Vagal Nerve and Carotid Body Stimulators for Cardiovascular Disease
In additional to proximal effects on the brain, the vagus nerve controls autonomic functions including heart rate, respiration, and vasomotor activity). These parasympathetic functions of the vagus are complemented/balanced by the activity of the nearby sympathetic chain that includes carotid body baroreceptors. Accordingly, electrical stimulation of both the vagus and carotid body have been used to treat drug-refractory hypertension and heart failure. Two such neurostimulators are currently marketed:
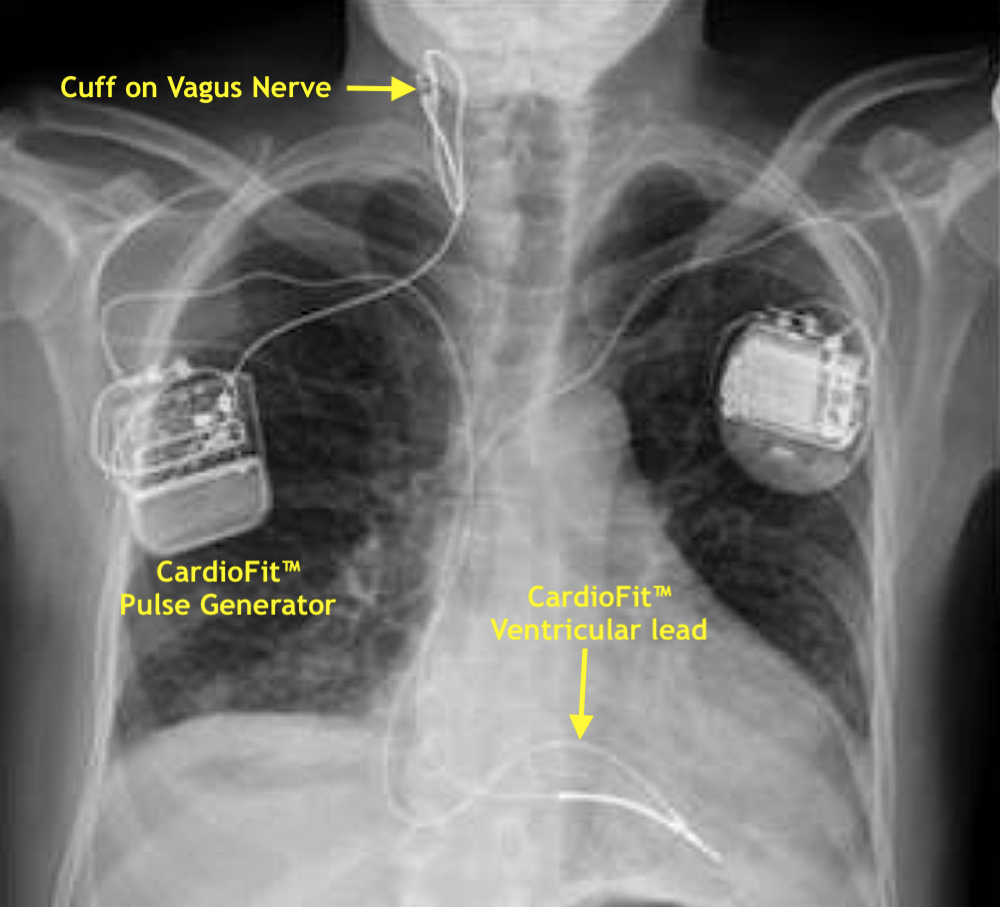 CardioFit™ Vagal Nerve Stimulator
CardioFit™ Vagal Nerve Stimulator
The CardioFit™ (BioControl Medical), available in Europe but not the US, is a vagal nerve stimulator originally tested for neurologic disorders but now marketed for drug-refractory heart failure. The pulse generator is implanted subcutaneously in the right upper chest with two leads: 1) a sensing electrode with tip in the right ventricle, and 2) a stimulating electrode on a cuff placed around the right vagus nerve. The CardioFit™ fared poorly in a recent multi-center trial and has received CE mark (for sale in Europe) but not US-FDA approval. The manufacturer has provided no testing data, so for now the CardioFit™ must be considered MR Unsafe.
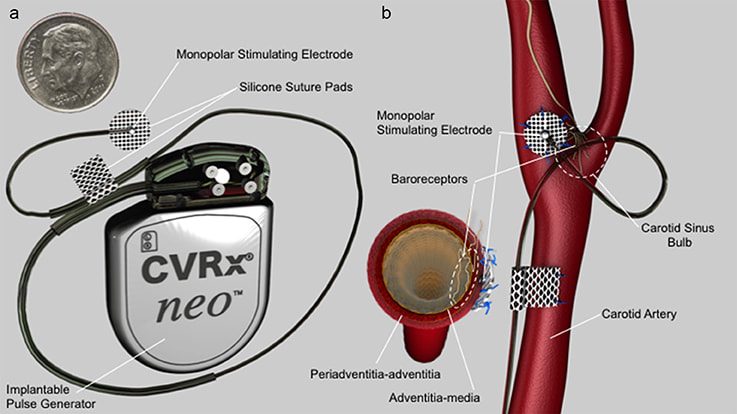 Barostim Neo™ System (from Wilks et al under CC-BY)
Barostim Neo™ System (from Wilks et al under CC-BY)
The Barostim Neo™ (CVRx) stimulates the baroreceptors of the sympathetic nervous system. A titanium-encased pulse generator is subcutaneously implanted in the upper chest with a lead tunneled through the neck to terminate at the carotid sinus (at the common carotid artery bifurcation). Continuous current stimulates the carotid baroreceptors, which in turn lower blood pressure, decrease heart rate, and improve renal excretion. Older versions (Rheos™ and Barostim™ Legacy 2100) are MR Unsafe, but the newer Barostim Neo™ Model 2102 is MR Conditional at 1.5T. Restrictions and precautions similar to the LivaNova VNS must be followed, including pre- and post-MRI reprogramming, SAR limits, and exclusion of the device from direct RF body coil stimulation.
References
Anand IS, Konstam MA, Klein HU, et al. Comparison of symptomatic and functional responses to vagus nerve stimulation in ANTHEM-HF, INOVATE-HF and NECTAR-HF. ESC Heart Failure 2020; 7:76-84. [DOI LINK]
CVRx, Inc. MRI Use Instructions (for BarostimNeo). August 2019. (Before scanning always check manufacturer's web site for most recent version of this document and current recommendations)
LivaNova. MRI with the VNS Therapy® System. October 2019. (Before scanning always check manufacturer's web site for most recent version of this document and current recommendations)
Vaughan JT, Adrian G, Snyder CJ, et al. Efficient high-frequency body coil for high-field MRI. Magn Reson Med 2004; 52:851-859. [DOI LINK]
Wilks SJ, Hara SA, Ross EK, et al. Non-clinical and pre-clinical testing to demonstrate safety of the Barostim Neo electrode for activation of carotid baroreceptors in chronic human implants. Front Neurosci 2017; 11:438. [DOI LINK]
Anand IS, Konstam MA, Klein HU, et al. Comparison of symptomatic and functional responses to vagus nerve stimulation in ANTHEM-HF, INOVATE-HF and NECTAR-HF. ESC Heart Failure 2020; 7:76-84. [DOI LINK]
CVRx, Inc. MRI Use Instructions (for BarostimNeo). August 2019. (Before scanning always check manufacturer's web site for most recent version of this document and current recommendations)
LivaNova. MRI with the VNS Therapy® System. October 2019. (Before scanning always check manufacturer's web site for most recent version of this document and current recommendations)
Vaughan JT, Adrian G, Snyder CJ, et al. Efficient high-frequency body coil for high-field MRI. Magn Reson Med 2004; 52:851-859. [DOI LINK]
Wilks SJ, Hara SA, Ross EK, et al. Non-clinical and pre-clinical testing to demonstrate safety of the Barostim Neo electrode for activation of carotid baroreceptors in chronic human implants. Front Neurosci 2017; 11:438. [DOI LINK]
Related Questions
What precautions must be taken when scanning patients with an InterStim device?
Can patients with deep brain stimulators be scanned?
What precautions must be taken when scanning patients with an InterStim device?
Can patients with deep brain stimulators be scanned?