ASL Artifacts
What ASL artifacts should we know about?
|
|
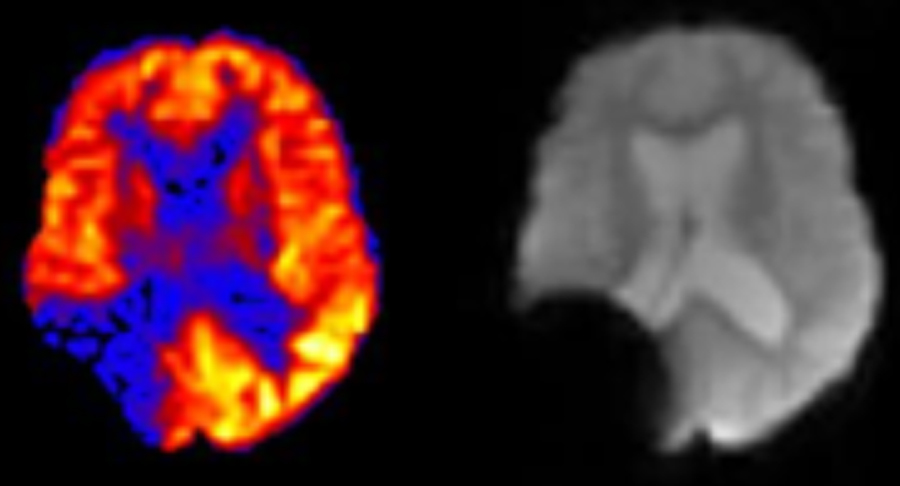
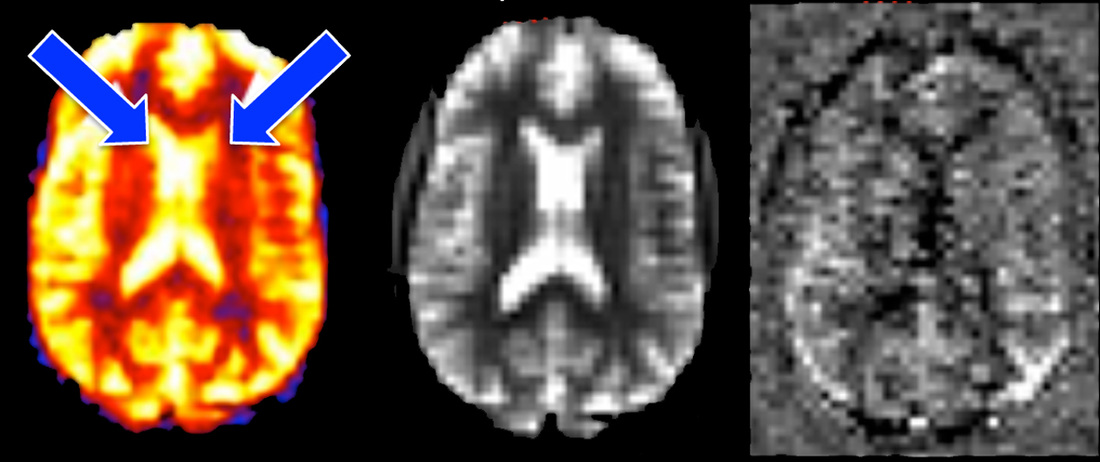
Susceptibility artifact mimicking area of hypoperfusion on ASL
|
Susceptibility artifact. ASL suffers from the same artifacts as other MR techniques, including susceptibility, flow, and motion. However, some of these problems manifest differently on ASL than on conventional images. In the figure left we see a susceptibility artifact easily recognized on the source image that mimics a region of hypoperfusion/infarct on the ASL image.
|
|
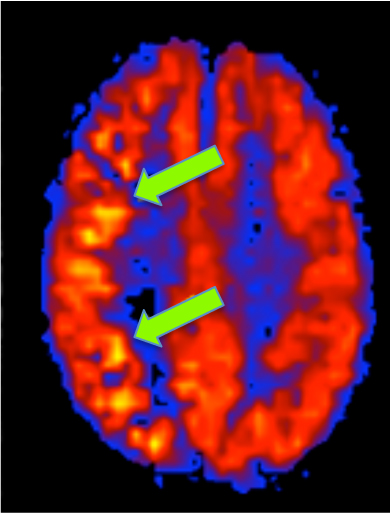
Coil sensitivity artifact. Spatial variations in receiver coil sensitivity may also mimic areas of hyper- or hypo-perfusion on ASL images. In the figure right, spurious increased perfusion is suggested (arrows), whose true nature is recognized by inspecting the source images. Coil artifacts may be mitigated by image filtering and other postprocessing techniques.
|
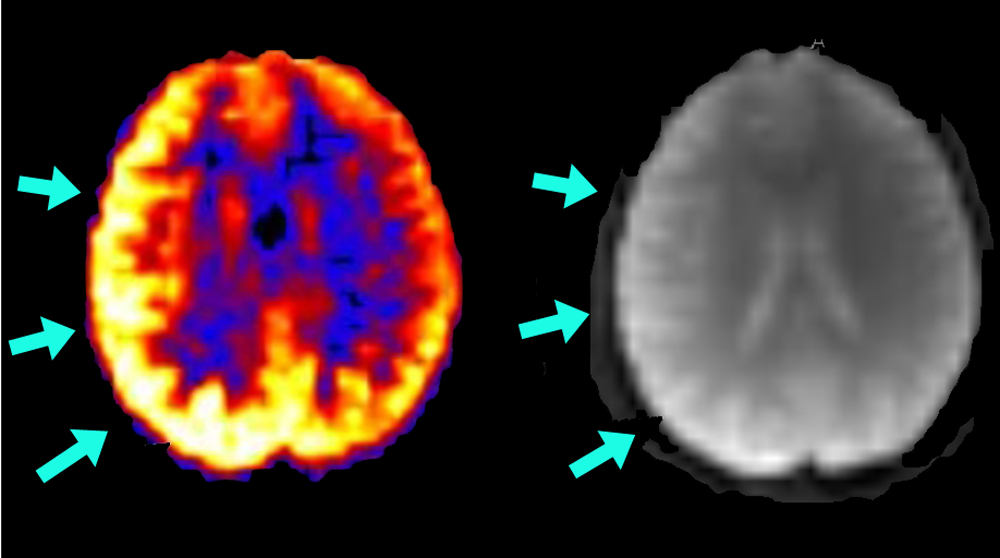
Coil sensitivity artifact
|
Motion artifact on successive ASL slices manifest by varying contrast and bright halo at edge of images.
|
Motion artifact. Patient movement between control and tagging sequences often appears as a halo around the area of interest. In brain ASL this is typically manifest by visualization of the scalp. Slice-to-slice variations in brightness may also occur. Post processing motion correction is commonly performed to align the paired images and reduce these effects of gross patient motion. Slices with large position changes can even be discarded with little decrease in SNR.
|
|
Downstream signal loss. A common feature of most ASL techniques is reduced signal in the slices the farthest downstream (i.e., most distal from the inversion slab). This signal loss results from T1-relaxation of labeled protons between inversion and readout. The phenomenon is more noticeable at 1.5T than 3.0T because intrinsic blood T1 values are shorter at lower fields. The artifact can be reduced by using a 3D readout and parallel imaging techniques to shorten image acquisition time.
|
Downstream signal loss in higher slices
|
|
Intravacular signal artifact. Late arriving labeled spins may not have had time to diffuse into tissue and still be present in larger arteries at the time of imaging. This may occur if the inverted bolus is not sharply delineated during the labeling process, the inversion time (TI) is too short, or when there is pathological delayed arrival of the arterial bolus.
|
|
Large vessel signals can be recognized on perfusion images as exceptionally bright spots on the surface of the brain or other organs. In the images above we see signal in the right middle cerebral artery (blue arrow, left image) and in the superior sagittal sinus (white arrow, right image).
|
To reduce large vessel signals, large bipolar crusher gradients are often applied along several axes immediately prior to the image readout. Consideration must also be given to the optimal choice of TI, which depends on expected vascular flow rates. TI must be shorter in pediatric patients and longer in the elderly. Although usually a pesky artifact, persistent high vascular signal on ASL can be a useful clinical sign, reflecting delayed arterial transit from vascuar disease. The image right shows high ASL signal in cerebral arteries in a patient with sluggish flow due to longstanding internal carotid artery occlusion.
|
Arterial signals in patient with carotid occlusion
|
|
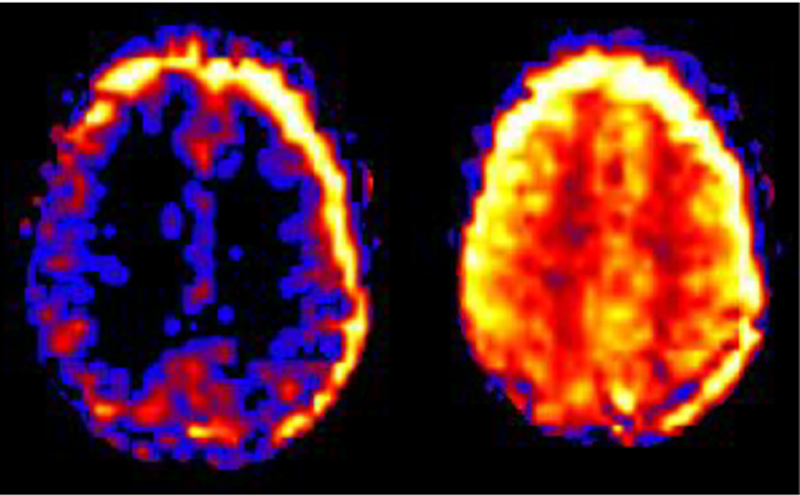
Failed Background suppression. Because the differences in MR signal between tagged and control sequences are small, any motion or other changes in the background tissue can overwhelm the perfusion weighted images with noise and artifacts. This is especially true for 3D ASL methods. To reduce these effects, most clinical ASL sequences employ some type of background suppression of the imaged volume.
|
Failed background suppression in ASL image shows abnormal high signal in ventricles (arrows) due to T2-shine-through effects. The raw data images shows how background suppression failed on the control image (middle) but not the tagged image (right).
|
The usual method is to apply additional slice-specific inversion or saturation pulses to stationary tissue while leaving the flow sensitive component relatively unaffected. If background saturation fails during part of an ASL examination, postprocessing methods may identify and discard the affected slices, thus salvaging an otherwise unreadable exam.
References
Amukotuwa SA, Yu C, Zharchuk G. 3D Pseudocontinuous Arterial Spin Labeling in routine clinical practice: a review of clinically significant artifacts. J Magn Reson Imaging 2016; 43:11-27 (good recent review)
Diebler AR, Pollock JM, Kraft RA, et al. Arterial spin-labeling in routine clinical practice, Part 1: techniques and artifacts. AJNR Am J Neuroradiol 2008; 29:1228-1234.
Petersen ET, Zimine I, Ho Y-C L, Golay X. Non-invasive measurement of perfusion: a critical review of arterial spin labelling techniques. Br J Radiol 2006; 79:688-701.
Ye FQ, Mattay VS, Jezzard P, et al. Correction for vascular artifacts in cerebral blood flow values measured by using arterial spin tagging techniques. Magn Reson Med 1997; 37:226–235. (use of bipolar crusher gradients to suppress ASL signal in large arteries)
Amukotuwa SA, Yu C, Zharchuk G. 3D Pseudocontinuous Arterial Spin Labeling in routine clinical practice: a review of clinically significant artifacts. J Magn Reson Imaging 2016; 43:11-27 (good recent review)
Diebler AR, Pollock JM, Kraft RA, et al. Arterial spin-labeling in routine clinical practice, Part 1: techniques and artifacts. AJNR Am J Neuroradiol 2008; 29:1228-1234.
Petersen ET, Zimine I, Ho Y-C L, Golay X. Non-invasive measurement of perfusion: a critical review of arterial spin labelling techniques. Br J Radiol 2006; 79:688-701.
Ye FQ, Mattay VS, Jezzard P, et al. Correction for vascular artifacts in cerebral blood flow values measured by using arterial spin tagging techniques. Magn Reson Med 1997; 37:226–235. (use of bipolar crusher gradients to suppress ASL signal in large arteries)
Related Questions
Can gadolinium be given in conjunction with ASL?
Can gadolinium be given in conjunction with ASL?