Pseudo-Continuous Arterial Spin Labeling (pCASL)
What is pCASL and how does it differ from CASL and PASL?
|
|
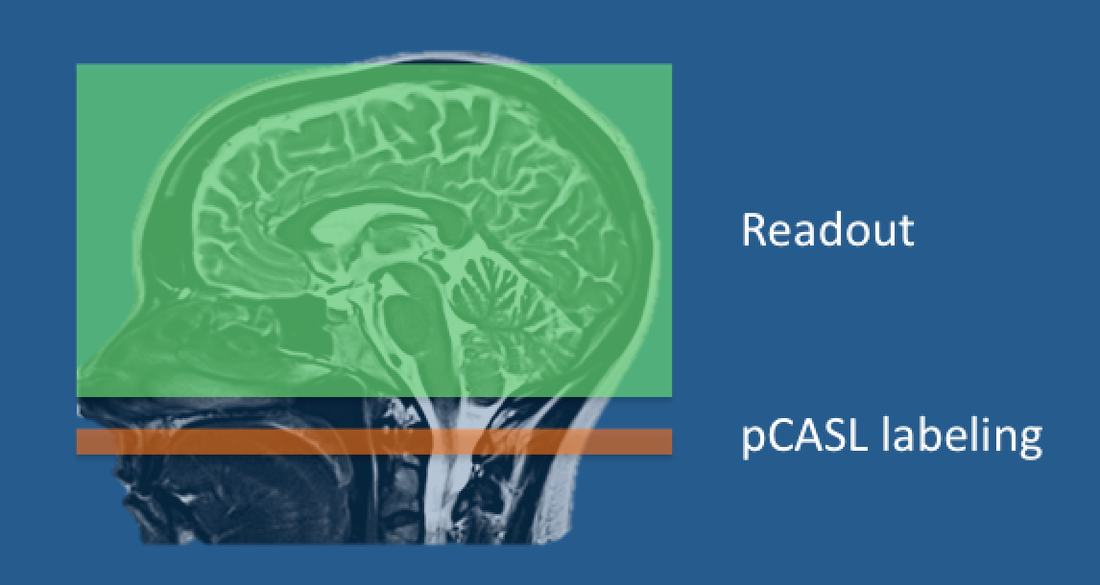 The pCASL technique with a narrow labeling band just
The pCASL technique with a narrow labeling band justproximal to the imaged volume
In 2008 Dai et al proposed a hybrid method between CASL and PASL named pCASL (Pseudo-Continuous Arterial Spin Labeling). pCASL uses a narrow labeling plane (similar to CASL) through which flow-related adiabatic inversion of arterial spins occurs. The tagging is performed immediately proximal to the imaging volume and thus minimizes signal loss from the decay of labeled blood. Unlike CASL where continuous RF-irradiation is used, pCASL uses a train of very short RF-pulses that mimic the action of a single long CASL pulse but with much lower energy deposition and RF-amplifier duty cycle requirements.
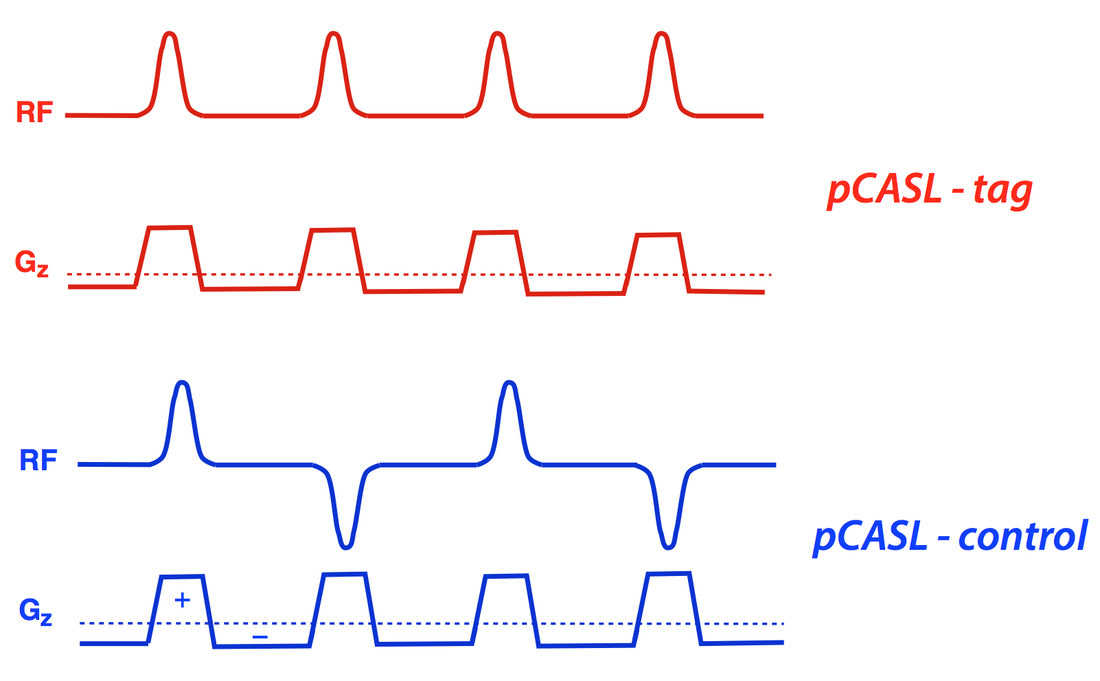 pCASL pulse sequence. In the tagging portion the slice-select
pCASL pulse sequence. In the tagging portion the slice-selectgradient (Gz) is unbalanced, but balanced in the control.
Alternating RF-phase is also used in the control portion.
In a typical implementation pCASL might use 750 Hanning-shaped 20° RF-pulses each lasting 0.5 msec applied over a 1.5 second period. The refocusing portion of the slice-selection gradient is unbalanced in the tagging sequence. This means that flowing spins will accumulate an additional phase offset during application of each RF-pulse. The control sequence uses balanced gradients to remove this effect. Additionally the phase of each RF-pulse in the control sequence is alternated.
Since its original description pCASL has become very popular and is currently our ASL method of choice. Compared to PASL, pCASL offers higher SNR and is less sensitive to tag dispersion. Compared to CASL, pCASL offers higher labeling efficiency and can be implemented on modern clinical scanners with only software modifications. The tagging efficiency of pCASL, however, is not as great as PASL, and is highly sensitive to flow velocity, angle of flow, and B1 and Bo inhomogeneities.
References
Dai W, Garcia D, de Bazelaire C, Alsop DC. Continuous flow driven inversion for arterial spin labeling using pulsed radiofrequency and gradient fields. Magn Reson Med 2008; 60:1488-1497. (original description of pCASL)
Golay X, Hendrikse J, Lim TCC. Perfusion imaging using arterial spin labeling. Top Magn Reson Imaing 2004; 15:10-27. (Good review plus a description of ASL of variants and acronyms such as FAIRER, TILT, BASE, and others).
Kober F, Jan T, Trollen, Kayak KS. Myocardial arterial spin labeling. J Cardiovasc Magn Reson 2016; 18:22. (Primary focus is on the Look-Locker FAIR techniques most widely used in cardiac ASL)
Luh W-M, Wong EC, Bandettini PA, Hyde JS. QUIPSS II with thin-slice TI1 periodic saturation: a method for improving accuracy of quantitative perfusion imaging using pulsed arterial spin labeling. Magn Reson Med 1999; 41:1246-1254.
Petersen ET, Lim T, Golay X. Model-free arterial spin labeling quantification: approach for perfusion MRI. Magn Reson Med 2006; 55:219-232. (QUASAR method)
Wong EC, Buxton RB, Frank LR. Quantitative imaging of perfusion using single subtraction (QUIPSS and QUIPSS II). Magn Reson Med 1998; 39:702-708.
Dai W, Garcia D, de Bazelaire C, Alsop DC. Continuous flow driven inversion for arterial spin labeling using pulsed radiofrequency and gradient fields. Magn Reson Med 2008; 60:1488-1497. (original description of pCASL)
Golay X, Hendrikse J, Lim TCC. Perfusion imaging using arterial spin labeling. Top Magn Reson Imaing 2004; 15:10-27. (Good review plus a description of ASL of variants and acronyms such as FAIRER, TILT, BASE, and others).
Kober F, Jan T, Trollen, Kayak KS. Myocardial arterial spin labeling. J Cardiovasc Magn Reson 2016; 18:22. (Primary focus is on the Look-Locker FAIR techniques most widely used in cardiac ASL)
Luh W-M, Wong EC, Bandettini PA, Hyde JS. QUIPSS II with thin-slice TI1 periodic saturation: a method for improving accuracy of quantitative perfusion imaging using pulsed arterial spin labeling. Magn Reson Med 1999; 41:1246-1254.
Petersen ET, Lim T, Golay X. Model-free arterial spin labeling quantification: approach for perfusion MRI. Magn Reson Med 2006; 55:219-232. (QUASAR method)
Wong EC, Buxton RB, Frank LR. Quantitative imaging of perfusion using single subtraction (QUIPSS and QUIPSS II). Magn Reson Med 1998; 39:702-708.
Related Questions
Can you briefly explain the difference between the various ASL methods? Which is the best?
Can you briefly explain the difference between the various ASL methods? Which is the best?