MRA with ASLWhat is arterial spin labeling (ASL) and how does it improve MRA?
|
|
Arterial spin labeling (ASL) methods use RF-pulses to magnetically "tag" protons in arterial blood prior to their entry into an organ or capillary bed. When these labeled water protons enter a new anatomic region they can be recognized by their unique magnetic signature and used to produce an arteriogram. ASL was originally developed to measure tissue perfusion, the subject of several later Q&A's, but here the focus is on its use in MR angiography.
The simplest form of MRA with ASL is called the Outflow Method. The sequence begins with two 180°-RF pulses applied in close succession. The first 180°-pulse is non-selective, meaning it inverts the entire background regardless of location. The second 180°-pulse is spatially-selective, applied to restore magnetization in the region from which the "fresh" blood will flow. During the inversion time (TI) interval, this fully magnetized ("fresh") blood will enter the anatomic area of interest. Signal generation is then initiated using either a 3D balanced-SSFP or FSE sequence to produce the MRA.
In brief, two phenomena are occurring simultaneously during the inversion period of the MRA-ASL sequence. Stationary tissue, whose magnetization has been initially inverted by the first nonselective 180°-pulse, is recovering via T1-relaxation back toward zero. Tagged blood, whose magnetization has been restored to Mo by the second 180°-pulse, is flowing out of the tag region into the imaging volume. TI is chosen to coincide with the null point for stationary tissues, which at 1.5 is typically in the 1000-1200 msec range.
|

ASL Outflow method for portal MR venography. Blood within the "Selective" area receives two 180°-pulses and is tagged (non-suppressed) producing signal during MRA readout.
|
As with other MRA methods, many variations are possible. These include applying additional saturation pulses to suppress signals from the aorta or vena cava. Canon offers ASL-MRA with a "Tag-on/Tag-off" option using image subtraction to improve background suppression. Separate arterial and venous images are also possible. These features come at the expense of increased imaging time and motion artifacts due to image subtraction.
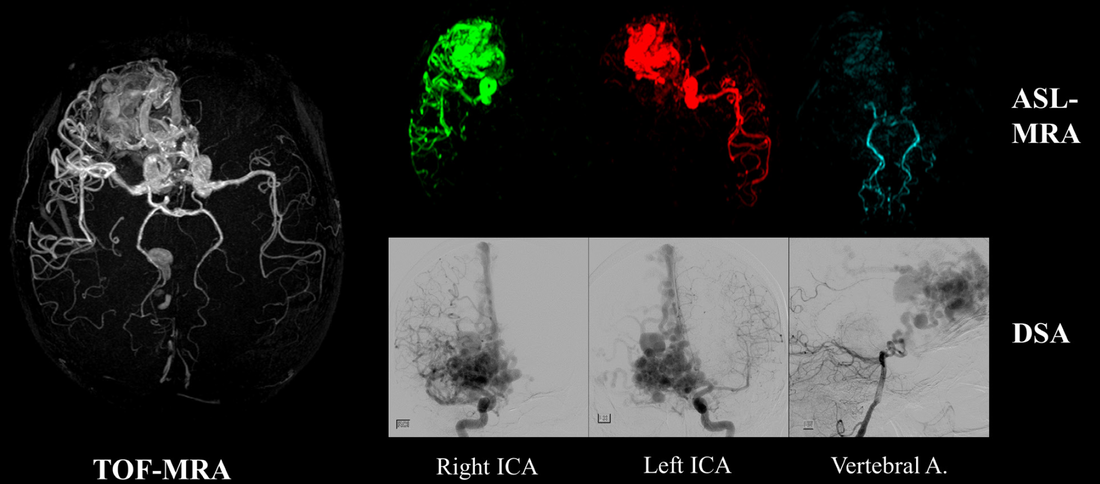
Vessel-selective 3D ASL-MRA applied to an arteriovenous malformation showing contributions to the nidus from each major vascular supply (from Suzuki under CC-BY)
ASL has several intrinsic limitations, and is not currently as widely used as many other MRA techniques. First, because ASL-MRA relies on the replacement of saturated blood by tagged blood, reasonably high arterial velocities are required for success. ASL methods may thus not be suitable for MRA of vessels with significant stenoses. ASL-MRA also presumes the flow direction is known, which may not always be the case, again with diseased vessels where retrograde collateral flow may be present.
References
Albert T, Kelly E. Time-Spatial labeling inversion pulse. Safe, simple and effective non-contrast MR angiography. From www.medical.toshiba.com, 2010.
Miyazaki M, Lee VS. Nonenhanced MR angiography. Radiology 2008;248:20-43.
Shimada T, Amanuma M, Takahasi A, Tsushima Y. Non-contrast renal MR angiography: value of subtraction of tagging and non-tagging technique. Ann Vasc Dis 2012; 5:161-165.
Suzuki Y, Fujima N, van Osch MJP. Intracranial 3D and 4D MR angiography using arterial spin labeling: technical considerations. Magn Reson Med Sci 2020; 19:294-309. [DOI LINK]
Albert T, Kelly E. Time-Spatial labeling inversion pulse. Safe, simple and effective non-contrast MR angiography. From www.medical.toshiba.com, 2010.
Miyazaki M, Lee VS. Nonenhanced MR angiography. Radiology 2008;248:20-43.
Shimada T, Amanuma M, Takahasi A, Tsushima Y. Non-contrast renal MR angiography: value of subtraction of tagging and non-tagging technique. Ann Vasc Dis 2012; 5:161-165.
Suzuki Y, Fujima N, van Osch MJP. Intracranial 3D and 4D MR angiography using arterial spin labeling: technical considerations. Magn Reson Med Sci 2020; 19:294-309. [DOI LINK]
Related Questions
How do inflow-enhanced SSFP MRA sequences work? Where do you place the saturation bands?
What is arterial spin labeling (ASL) and how does it work?
How do inflow-enhanced SSFP MRA sequences work? Where do you place the saturation bands?
What is arterial spin labeling (ASL) and how does it work?