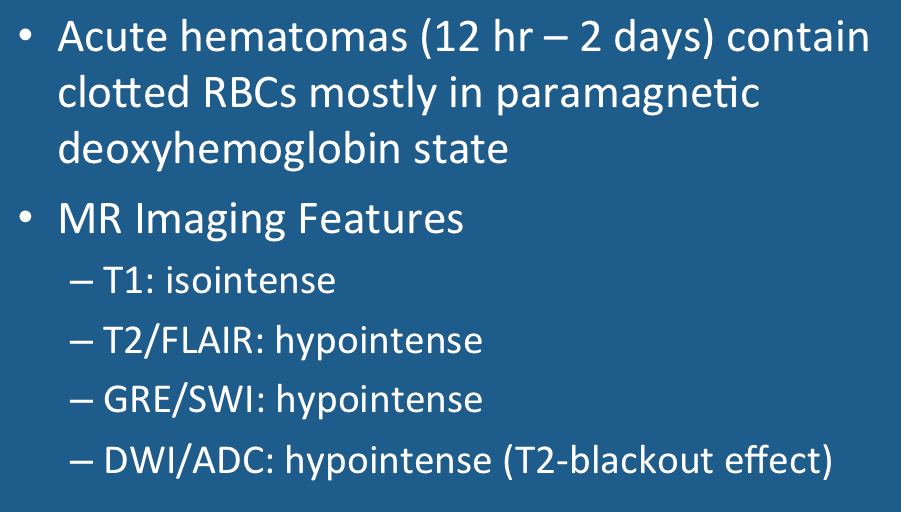
Acute Hemorrhage: Deoxyhemoglobin
Why does acute hemorrhage become dark on T2-weighted images?
|
|
Acute hemorrhage is arbitrarily defined to be bleeding between 12 hours and 2 days old. Hemorrhages occurring within the first 12 hours are called hyperacute, while those between 2 days and 2 months old are called subacute.

The stage of acute hemorrhage is characterized by robust formation of deoxyhemoglobin (deoxy-Hb), the hemoglobin species that has lost oxygen from its heme binding sites. Blood containing substantial quantities of deoxy-Hb is easily recognized by its dark purplish-red color, such as that seen in venous blood samples.
|

Loss of O2 to form deoxy-Hb results in conformational change of the hemoglobin molecule as well as profound alteration of its magnetic properties. (Image from the RCSB PDB www.rcsb.org; Click to animate).
|
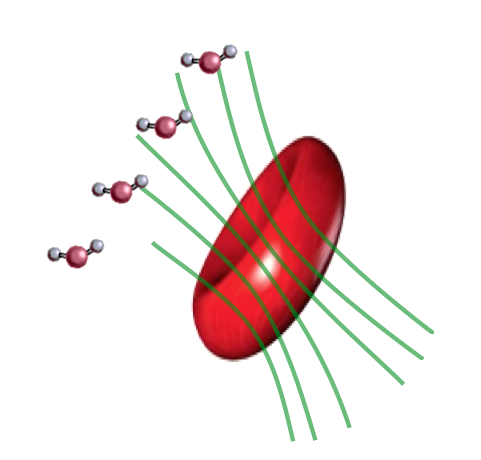 Local field distortions due to deoxy-Hb within
Local field distortions due to deoxy-Hb within RBCs dephases nearby H2O molecules, causing
loss of signal on T2/T2*-weighted images.
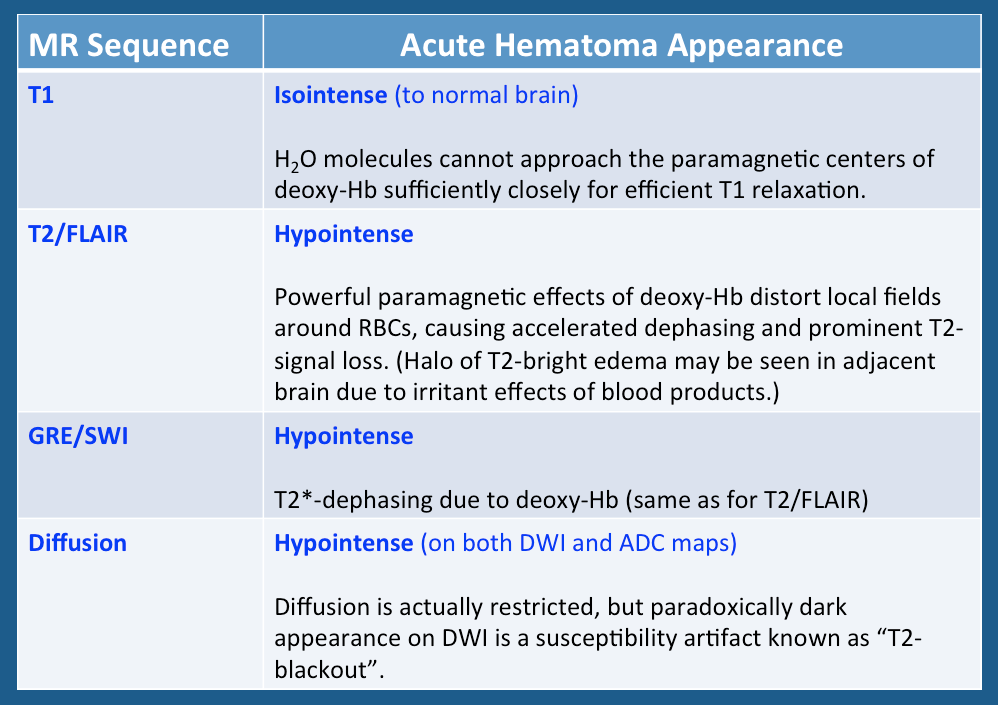
Deoxyhemoglobin formation typically begins at the periphery of a hematoma and gradually spreads inward. Deoxy-Hb, with 4 unpaired electrons per iron atom, is strongly paramagnetic. Because it is concentrated within RBCs, deoxy-Hb produces susceptibility-induced distortions of local magnetic fields. As water molecules diffuse past RBCs they encounter field variations on the order of 0.2-0.4 ppm. This results in accelerated dephasing and loss of signal on T2/T2*-weighted images.
This marked dephasing due to concentrated deoxy-Hb spills over into diffusion-weighted images, producing the so-called "T2-blackout effect." In reality, diffusion remains restricted in the center of acute hematomas, just as it does in hyperacute ones. However, the expected high signal on DW images representing restricted diffusion is masked by susceptibility-induced signal loss.
Although T2 and T2* are significantly shortened by the acute hematoma, T1 values are relatively unaffected. This is because the conformation of the globin proteins do not allow water molecules close access to the paramagnetic centers of deoxy-Hb. Outer sphere relaxation mechanisms predominate, resulting in strong effects on T2 with little or no change in T1 values. Thus, as with hyperacute hemorrhages, T1-weighted images remain isointense to brain.
This marked dephasing due to concentrated deoxy-Hb spills over into diffusion-weighted images, producing the so-called "T2-blackout effect." In reality, diffusion remains restricted in the center of acute hematomas, just as it does in hyperacute ones. However, the expected high signal on DW images representing restricted diffusion is masked by susceptibility-induced signal loss.
Although T2 and T2* are significantly shortened by the acute hematoma, T1 values are relatively unaffected. This is because the conformation of the globin proteins do not allow water molecules close access to the paramagnetic centers of deoxy-Hb. Outer sphere relaxation mechanisms predominate, resulting in strong effects on T2 with little or no change in T1 values. Thus, as with hyperacute hemorrhages, T1-weighted images remain isointense to brain.
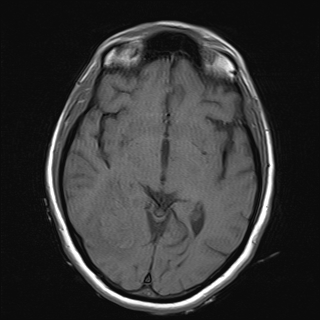
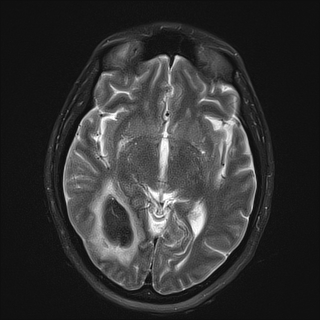
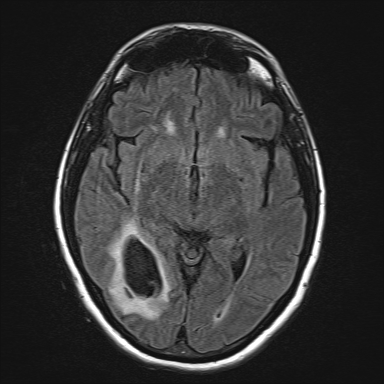
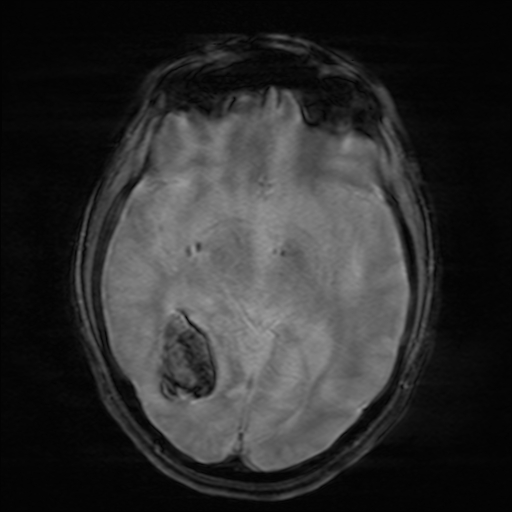
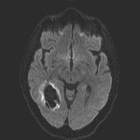
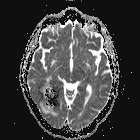
Above: MR images obtained about 18 hours after hemorrhage with prominent deoxyhemoglobin formation. Hematoma is isointense to brain on T1-weighted image (top left). Center of hematoma is markedly hypointense on T2 (top center) and T2-FLAIR (top right) images. A halo of high signal edema in the surrounding brain is noted. GRE image (bottom left) shows loss of signal due to T2* dephasing from paramagnetic deoxy-Hb confined to RBCs. DW image (bottom center) and ADC map (bottom right) both have dark centers, due to strong paramagnetic artifacts and the T2-blackout effect. Susceptibility artifacts make accurate calculation of ADC values difficult (manifest by specked appearance)
Important Note: The discussion above primarily applies to higher field (≥ 0.5 T) systems where imaging findings are dominated by the paramagnetic effects of hemoglobin. At low and intermediate fields some important differences in imaging appearances are noted. See this Q&A for a more detailed analysis.
References
Bradley WG Jr. MR appearance of hemorrhage in the brain. Radiology 1993; 189:15-26.
Gomori JM, Grossman RI. Mechanisms responsible for the MR appearance and evolution of intracranial hemorrhage. Radiographics 1988; 8:427-440.
Hiwatashi A, Kinoshita T, Moritani T et-al. Hypointensity on diffusion-weighted MRI of the brain related to T2 shortening and susceptibility effects. AJR Am J Roentgenol 2003; 181:1705-9.
Maldjian JA, Listerud J, Moonis G, Siddiqi F. Computing diffusion rates in T2-dark hematomas and areas of low T2 signal. AJNR Am J Neuroradiol 2001;22:112–128.
Silvera S, Oppenheim C, Touzé E, et al. Spontaneous intracerebral hematoma on diffusion-weighted images: influence of T2-shine-through and T2-blackout effects. AJNR Am J Neuroradiol 2005; 26:236-241.
Bradley WG Jr. MR appearance of hemorrhage in the brain. Radiology 1993; 189:15-26.
Gomori JM, Grossman RI. Mechanisms responsible for the MR appearance and evolution of intracranial hemorrhage. Radiographics 1988; 8:427-440.
Hiwatashi A, Kinoshita T, Moritani T et-al. Hypointensity on diffusion-weighted MRI of the brain related to T2 shortening and susceptibility effects. AJR Am J Roentgenol 2003; 181:1705-9.
Maldjian JA, Listerud J, Moonis G, Siddiqi F. Computing diffusion rates in T2-dark hematomas and areas of low T2 signal. AJNR Am J Neuroradiol 2001;22:112–128.
Silvera S, Oppenheim C, Touzé E, et al. Spontaneous intracerebral hematoma on diffusion-weighted images: influence of T2-shine-through and T2-blackout effects. AJNR Am J Neuroradiol 2005; 26:236-241.
Related Questions
What are the different forms of hemoglobin and why do they have different magnetic properties?
I know what T2-shine-through is, but what is T2-blackout?
How does the MR appearance of blood differ at low and very low magnetic fields?
What are the different forms of hemoglobin and why do they have different magnetic properties?
I know what T2-shine-through is, but what is T2-blackout?
How does the MR appearance of blood differ at low and very low magnetic fields?