Cardiac MR Protocols
Our cardiac MRI binder contains over a dozen different protocols. Can you make sense of these?
|
|
As Cardiac Magnetic Resonance (CMR) has become increasingly more sophisticated, most centers have developed a relatively large number of imaging protocols tailored to specific clinical indications. As an overview, these may be divided in morphology, function, and viability studies.
Morphology (Anatomy)
Anatomic images of the heart and great vessels are a standard part of nearly every CMR examination. Such views are, of course, essential in patients with complex congenital malformations, but are needed even in morphologically "normal" patients due natural variability in heart size, position, and rotation.
Anatomic images of the heart and great vessels are a standard part of nearly every CMR examination. Such views are, of course, essential in patients with complex congenital malformations, but are needed even in morphologically "normal" patients due natural variability in heart size, position, and rotation.
In addition to conventional (axial, coronal, or sagittal views), several special oblique planes of imaging are routinely obtained for most cardiac studies. These may include long axis, short axis, and views of the valves, coronary arteries, and great vessels.
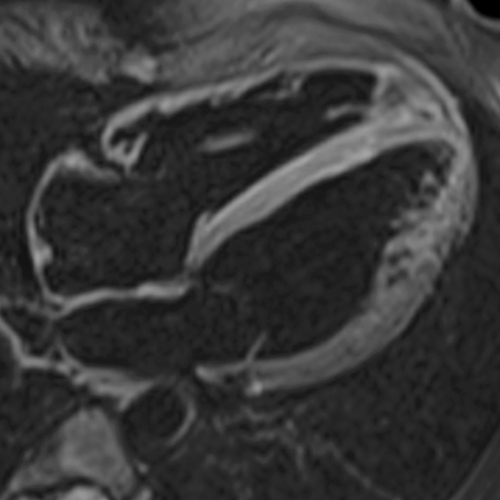


Two types of sequences are commonly used for morphologic imaging: dark blood and bright blood. Both are typically performed at multiple slice locations during diastole, producing a stack of images covering the relevant anatomy in 4-5 mm sections.
Dark ("black") blood sequences are utilize Inversion recovery (IR) prepulses to null the signal from blood alone (double IR), or from both blood and fat (triple IR). Rapid signal generation is usually based upon variants of the HASTE (Half-Fourier Acquisition Single-shot Turbo spin Echo) technique.
Bright blood sequences are typically based on b-SSFP (balanced Steady-State Free Precession) methods, perhaps better known by their vendor-specific nomenclature: TrueFISP (Siemens), FIESTA (GE), or b-FFE (Philips). These sequences reflect the relatively high T2/T1 ratio of blood.
Dark ("black") blood sequences are utilize Inversion recovery (IR) prepulses to null the signal from blood alone (double IR), or from both blood and fat (triple IR). Rapid signal generation is usually based upon variants of the HASTE (Half-Fourier Acquisition Single-shot Turbo spin Echo) technique.
Bright blood sequences are typically based on b-SSFP (balanced Steady-State Free Precession) methods, perhaps better known by their vendor-specific nomenclature: TrueFISP (Siemens), FIESTA (GE), or b-FFE (Philips). These sequences reflect the relatively high T2/T1 ratio of blood.
|
Cardiac Function (Motion)
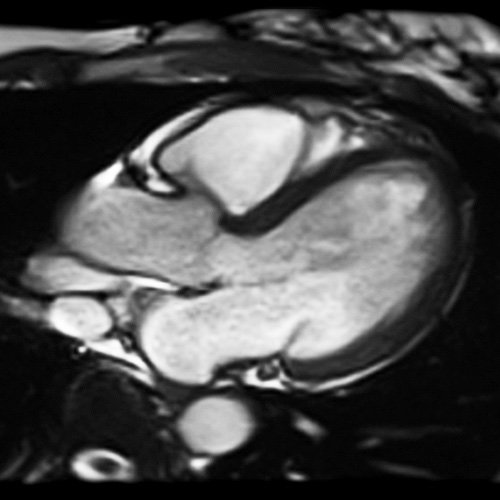
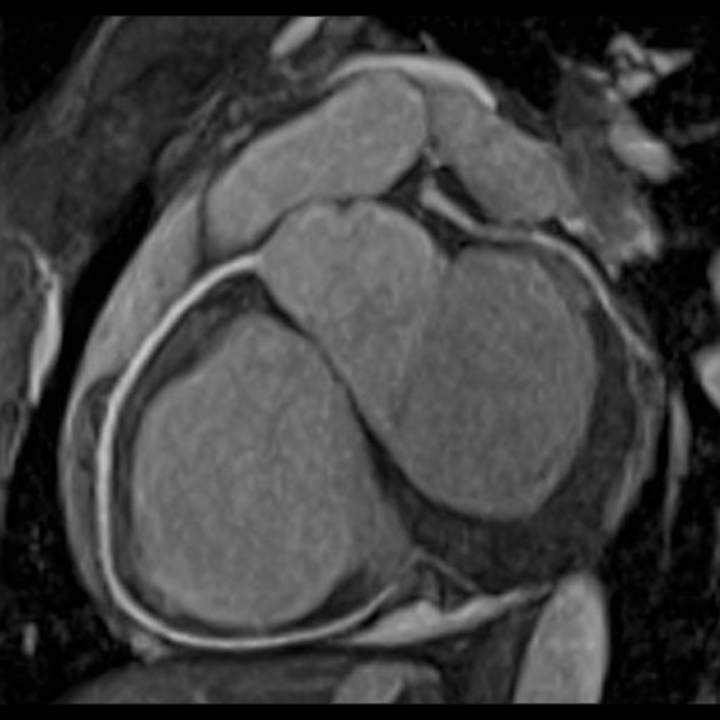
SSFP-based bright-blood images of the beating heart are essential for displaying cardiac function and are part of nearly every CMR examination. The motion of the ventricular walls during systole and diastole is of fundamental interest; this can be assessed both qualitatively and quantitatively. Additional information about valve function is also possible. The turbulence created by valvular stenosis or insufficiency creates loss of signal in the bright blood in proportion to its severity.
|
SSFP cine cardiac function study
|
Cine studies are obtained by repeatedly imaging the heart at a single slice location throughout the cardiac cycle. Between 16 and 32 cardiac phases are usually sampled and displayed in a movie loop. Data collection takes place over multiple cardiac cycles using retrospective EKG-gating and breath-holding. In sick or uncooperative patients, real-time cine images may be obtained in just a few milliseconds without breath-holding, but suffer from decreased spatial and temporal resolution.
|
Myocardial Viability/Perfusion
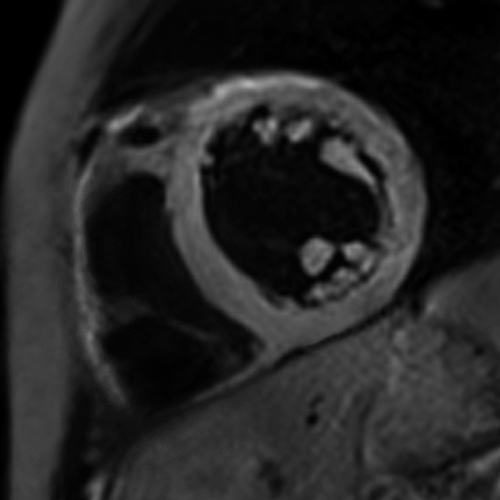
Myocardial viability is assessed using gadolinium-enhanced imaging. The standard methods utilize segmented, T1-weighted, inversion-prepared fast gradient echo sequences. The inversion time (TI) is chosen to null signal from myocardium, typically in the range of 250-350 ms at 1.5T. Precontrast images are first obtained followed by injection of half-dose gadolinium with first-pass perfusion imaging. An additional half- dose of gadolinium is then injected, with delayed images obtained at 10 and 20 minutes. Delayed enhancement is characteristic of subacute myocardial infarction, but also a number of other diseases.
|
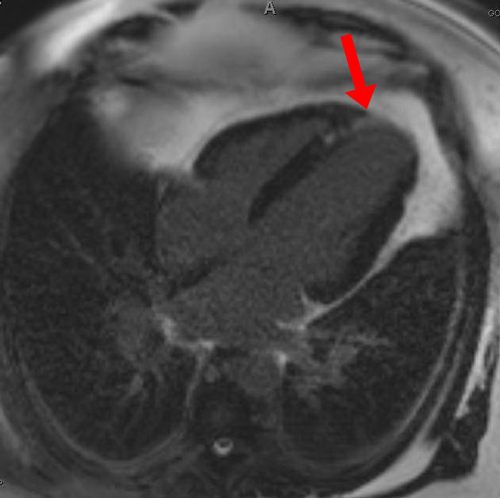
Delayed enhancement (arrow) in apical infarction
|
The sensitivity of gadolinium-enhanced CMR can be improved by combining first pass cine perfusion and delayed imaging in conjunction with pharmacological stress testing. In the past dobutamine was commonly used for this purpose, but now it has been largely replaced by adenosine or regadenoson.
You may find the YouTube videos and references below helpful in providing more information about the types of CMR pulse sequences available. These techniques will also be thoroughly explored in multiple subsequent Q&A's.
|
|
|
|
References
Fratz S, Chung T, Greil GF, et al. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson 2013; 15:51
Ginat DT, Fong MW, Tuttle DJ, et al. Cardiac imaging: Part I, MR pulse sequences, imaging planes, and basic anatomy. AJR Am J Roentgenol 2011; 197:808-815.
Herzog B, Greenwood J, Plein S. Cardiovascular magnetic resonance pocket guide, 2013. (A truly great booklet that includes protocols as well as normative values. You must read/review this!)
Hundley WG, Bluemke D, Bogaert JG, et al. Society for Cardiovascular Magnetic Resonance guidelines for reporting cardiovascular magnetic resonance examinations. J Cardiovasc Magn Reson 2009; 11:5.
Kawel-Boehm N, Maceira A, Valsangiacomo-Buechel, et al. Normal values for cardiovascular magnetic resonance in adults and children. J Cardiovasd Magn Reson 2015; 17:29 (extensive reference for normal measurements by MRI)
Kramer CM, Barkhausen J, Bucciarelli-Ducci C, et al. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J Cardiovasc Magn Reson 2020; 20:17. [DOI LINK]
Rajiah P, Bolen MA. Cardiovascular MR imaging at 3 T: opportunities, challenges, and solutions. RadioGraphics 2014; 34:1612-1635.
Raman SV, Markl M, Patel AR, et al. 30-minute CMR for common clinical indications: a Society for Cardiovascular Magnetic Resonance white paper. J Cardiovascular Magnet Resonance 2022:24:13. [DOI LINK]
Saremi F, Grizzard JD, Kim RJ. Optimizing cardiac MR imaging: Practical remedies for artifacts. RadioGraphics 2008; 28:1161-1187.
Schulz-Menger J, Bluemke DA, Bremerich J, et al. Standardized image interpretation and post processing in cardiovascular magnetic resonance: Society for Cardiovascular Magnetic Resonance (SCMR) Board of Trustees Task Force on Standardized Post Processing. J Cardiovasc Magn Reson 2013; 15:35.
Siemens. Cardiac Dot Protocols, 2015. SCMR Recommended Cardiac MRI Protocols, 2013. Available from this link at Siemens Medical. (About 20 cardiac protocols and how to perform them on various Siemens MR scanners).
Fratz S, Chung T, Greil GF, et al. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson 2013; 15:51
Ginat DT, Fong MW, Tuttle DJ, et al. Cardiac imaging: Part I, MR pulse sequences, imaging planes, and basic anatomy. AJR Am J Roentgenol 2011; 197:808-815.
Herzog B, Greenwood J, Plein S. Cardiovascular magnetic resonance pocket guide, 2013. (A truly great booklet that includes protocols as well as normative values. You must read/review this!)
Hundley WG, Bluemke D, Bogaert JG, et al. Society for Cardiovascular Magnetic Resonance guidelines for reporting cardiovascular magnetic resonance examinations. J Cardiovasc Magn Reson 2009; 11:5.
Kawel-Boehm N, Maceira A, Valsangiacomo-Buechel, et al. Normal values for cardiovascular magnetic resonance in adults and children. J Cardiovasd Magn Reson 2015; 17:29 (extensive reference for normal measurements by MRI)
Kramer CM, Barkhausen J, Bucciarelli-Ducci C, et al. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J Cardiovasc Magn Reson 2020; 20:17. [DOI LINK]
Rajiah P, Bolen MA. Cardiovascular MR imaging at 3 T: opportunities, challenges, and solutions. RadioGraphics 2014; 34:1612-1635.
Raman SV, Markl M, Patel AR, et al. 30-minute CMR for common clinical indications: a Society for Cardiovascular Magnetic Resonance white paper. J Cardiovascular Magnet Resonance 2022:24:13. [DOI LINK]
Saremi F, Grizzard JD, Kim RJ. Optimizing cardiac MR imaging: Practical remedies for artifacts. RadioGraphics 2008; 28:1161-1187.
Schulz-Menger J, Bluemke DA, Bremerich J, et al. Standardized image interpretation and post processing in cardiovascular magnetic resonance: Society for Cardiovascular Magnetic Resonance (SCMR) Board of Trustees Task Force on Standardized Post Processing. J Cardiovasc Magn Reson 2013; 15:35.
Siemens. Cardiac Dot Protocols, 2015. SCMR Recommended Cardiac MRI Protocols, 2013. Available from this link at Siemens Medical. (About 20 cardiac protocols and how to perform them on various Siemens MR scanners).
Related Questions
Are there any special measures needed in preparing a patient for a cardiac MRI exam?
Are there any special measures needed in preparing a patient for a cardiac MRI exam?