Myocardial PerfusionHow does a myocardial perfusion study MRI work? Why would you want to do one?
|
|
Myocardial MR perfusion studies typically consist of approximately 50 rapidly-acquired, T1-weighted, cine images at 3-6 slice positions obtained during passage of a gadolinium contrast bolus. A single study may be performed in the resting state only, but often both stress and resting perfusion series are acquired back-to-back. Pharmacologic "stress" is created by intravenous infusion of a vasodilator (adenosine/regadenoson) or positive inotrope (dobutamine). Delayed post-enhancement images are also commonly obtained to assess the extent of damaged myocardium.
Cine perfusion study. Contrast passes through RV, then LV, and finally into the myocardium.
|
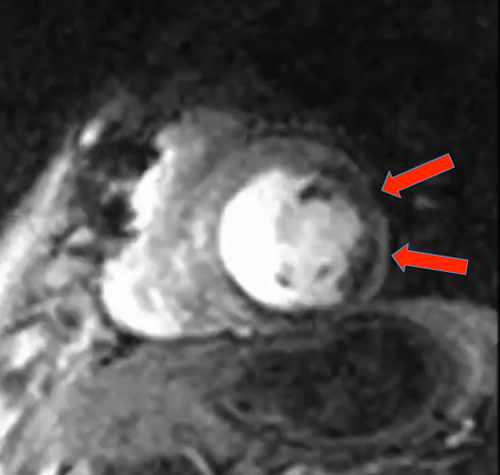
Single frame from cine study showing hypoperfusion (dark area, arrows) in the lateral wall
|
Stress perfusion MRI is typically performed in patients with known or suspected coronary atherosclerosis to identify areas of inducible ischemia, to predict cardiac prognosis, to stratify risk for non-cardiac surgery, or to assess myocardial viability. Contraindications for a stress study include recent (<3 days old) myocardial infarction, unstable angina, uncontrolled arrhythmias, aortic dissection or aneurysm, active myocarditis/pericarditis, severe hypertension (>225/120), severe aortic stenosis, and allergies to gadolinium or stressor agents.
|
In healthy persons the resistance of the coronary vascular bed is determined not by the larger (named) epicardial arteries, but by small (100−250 μm) intramural arterioles. These smaller vessels autoregulate myocardial flow by dilating in response to increased oxygen demand, local metabolites, and changes in blood pressure. The epicardial coronary arteries become flow-limiting only when narrowed by disease (atherosclerosis). The percent anatomic stenosis of a coronary artery is only a crude/imperfect predictor of clinical significance and response to therapy. For example, a 60% stenosis may not be symptomatic at rest, but become flow-limiting when the distal tree is maximally dilated.
|
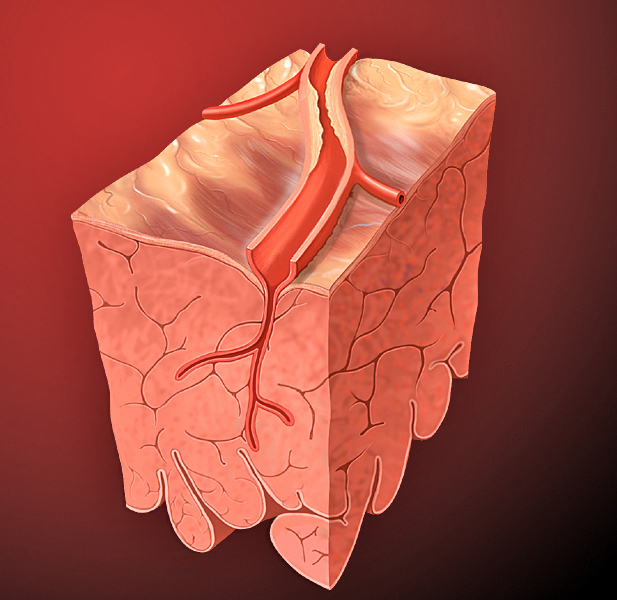
Resistance of coronary bed is determined by small intramural arterioles until large epicardial arteries become narrowed by atherosclerosis.
|
The dynamic nature of cardiac ischemia is reflected in the concept of coronary flow reserve (CFR), first proposed by Gould in 1974. CFR is a measure of the degree to which the coronary circulation is able to increase myocardial blood flow when the perfusion bed is maximally dilated. Normal values of CFR vary by age and sex but are typically in the range of 3-4; CFR values less than 2 are generally pathologic and associated with ischemia/infarction. Contrast-enhanced MRI performed at rest and under pharmacologic stress does not measure CFR directly, but a closely related quantity, myocardial flow reserve (MFR). Like CFR, MFR has been shown to be an important predictor for future coronary events in patients with coronary artery disease and outcomes after revascularization or stenting.
References
Carmici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med 2007; 356:830-40.
Duncker DJ, Koller A, Merkus D, Cantry JM. Regulation of coronary blood flow in health and ischemic heart disease. Prog Cardivasc Dis 2015; 52:409-422.
Gould KL, Kirkeeide RL, Buchi M. Coronary flow reserve as a physiologic measure of stenosis severity. J Amer Coll Cardiol 1990; 15:459-474.
Hundley WG, Morgan TM, Neagle CM, et al. Magnetic resonance imaging determination of cardiac prognosis. Circulation 2002; 106:2328-2333.
Shehata ML, Basha TA, Hayeri MR, et al. MR myocardial perfusion imaging: insights on techniques, analysis, interpretation, and findings. RadioGraphics 2014; 34:1636-1657.
Carmici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med 2007; 356:830-40.
Duncker DJ, Koller A, Merkus D, Cantry JM. Regulation of coronary blood flow in health and ischemic heart disease. Prog Cardivasc Dis 2015; 52:409-422.
Gould KL, Kirkeeide RL, Buchi M. Coronary flow reserve as a physiologic measure of stenosis severity. J Amer Coll Cardiol 1990; 15:459-474.
Hundley WG, Morgan TM, Neagle CM, et al. Magnetic resonance imaging determination of cardiac prognosis. Circulation 2002; 106:2328-2333.
Shehata ML, Basha TA, Hayeri MR, et al. MR myocardial perfusion imaging: insights on techniques, analysis, interpretation, and findings. RadioGraphics 2014; 34:1636-1657.
Related Questions
What is the best technique for "first pass" perfusion imaging?
What is the best technique for "first pass" perfusion imaging?