Slow Flow v Thrombus
How do you distinguish slow flow from thrombus on MR images?
|
|
|
This is a common problem that comes up several times a month at our institution. The most common locations are the transverse sinuses, jugular, femoral, and iliac veins. Fortunately, there are usually clues on routine imaging sequences, as well as special techniques that may help you resolve this dilemma.
|
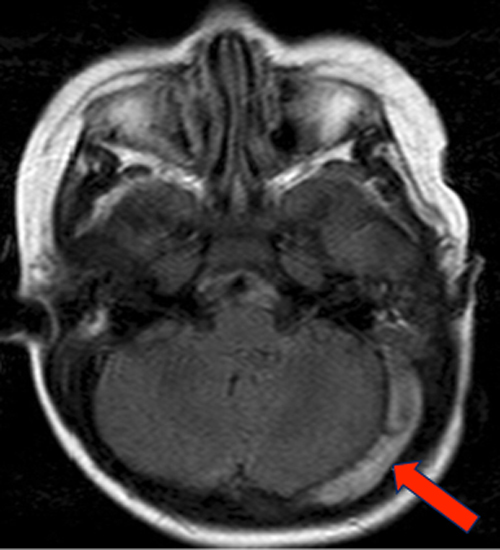
Pseudothrombosis in left transverse sinus due to sluggish flow
|

3D-TRICKS gadolinium-enhanced MR venogram confirms that the sinus is patent
|
The "thrombus vs slow flow" problem can usually be solved by non-MRI methods, such as CT venography or Doppler ultrasonography. Or the patient could be scheduled to return to the MR center for phase-contrast or gadolinium-enhanced venography, as shown in the example above.
If the patient is still in the scanner when the thrombosis question is raised, an argument might be made simply to perform a (usually) definitive contrast-enhanced MR venogram at the time. This may not be possible, however, for the following reasons: 1) the patient may have already received gadolinium; 2) gadolinium may be contraindicated because of allergy or renal insufficiency; and 3) insurance may not cover the additional study.
Often, however, the question of slow flow vs thrombosis arises after the study has been completed and the patient has left the MR Center. Of course, the patient could be called back for additional sequences, but why subject the patient to the extra time and expense of this when in most cases you can solve the problem by careful inspection of the images you have?
If the patient is still in the scanner when the thrombosis question is raised, an argument might be made simply to perform a (usually) definitive contrast-enhanced MR venogram at the time. This may not be possible, however, for the following reasons: 1) the patient may have already received gadolinium; 2) gadolinium may be contraindicated because of allergy or renal insufficiency; and 3) insurance may not cover the additional study.
Often, however, the question of slow flow vs thrombosis arises after the study has been completed and the patient has left the MR Center. Of course, the patient could be called back for additional sequences, but why subject the patient to the extra time and expense of this when in most cases you can solve the problem by careful inspection of the images you have?
Clues on Routine Imaging
The first step in differentiating between slow flow and thrombus is to look carefully at the area in question on all imaging sequences. It is particularly helpful if the same pulse sequence has been used in two different planes. With slow flow, the intravascular signal often changes when different imaging planes have been used; thrombus will have the same intensity regardless of the plane.
A second clue from routine imaging is to compare the signal of the questionable vessel on both T1- and T2-weighted images. Flow enhancement usually fades as TE is increased; thrombus is often of intermediate or high signal on all sequences. (If gradient-moment nulling was used on the long TE image, however, this trick will not work.)
If diffusion-weighted imaging or T2*/susceptibility-weighted imaging has been performed, these images may provide powerful information about the presence or absence of thrombosis. Generally, acute or subacute thrombus will be bright on DWI and dark on T2*/SWI images. Longstanding clot may not have these identifiable signal characteristics, however.
Is the abnormal intravascular signal maximal at the end slice, and does it fade out as one moves inward? Chances are you are dealing with inflow enhancement rather than thrombus.
Is there any evidence of phase artifacts (ghosting) adjacent to the vessel? (You may have to re-window the image and look in the air outside the patient to see it). If you do see ghosting, some flow must be present.
Does the area in question get brighter with gadolinium? Although gadolinium may diffuse into a clot, seeing a significantly brighter signal postcontrast supports the diagnosis of vascular patency. However, since tumor thrombi may enhance vividly with gadolinium, contrast enhancement will not aid much in the differential diagnosis in this scenario.
If the patient is still in the scanner at the time the questionable venous abnormality is noted a quick 2D phase-contrast MR venogram may be with a low velocity-encoding (VENC) gradient (e.g., 20 cm/sec). Slow flow will often become immediately apparent when this technique is used. Very slow flow may still be missed, however.
Another simple technique is to apply a presaturation band upstream from the site of suspected thrombosis. The signal from thrombus will be unaffected by this maneuver; flow signal will be reduced or eliminated.
Try repeating the T1- or T2-weighted images using a different plane of section than in the original. Slow flow may change its appearance, but thrombus will not.
Finally, consider repeating the sequences with and without gradient-moment nulling. Flow may change in appearance, thrombus will not.
If these techniques all fail, you may need to equivocate and recommend an additional MR, CT, or Doppler study to resolve the issue. With careful observations and employing the techniques above, this should only occasionally be necessary.
The first step in differentiating between slow flow and thrombus is to look carefully at the area in question on all imaging sequences. It is particularly helpful if the same pulse sequence has been used in two different planes. With slow flow, the intravascular signal often changes when different imaging planes have been used; thrombus will have the same intensity regardless of the plane.
A second clue from routine imaging is to compare the signal of the questionable vessel on both T1- and T2-weighted images. Flow enhancement usually fades as TE is increased; thrombus is often of intermediate or high signal on all sequences. (If gradient-moment nulling was used on the long TE image, however, this trick will not work.)
If diffusion-weighted imaging or T2*/susceptibility-weighted imaging has been performed, these images may provide powerful information about the presence or absence of thrombosis. Generally, acute or subacute thrombus will be bright on DWI and dark on T2*/SWI images. Longstanding clot may not have these identifiable signal characteristics, however.
Is the abnormal intravascular signal maximal at the end slice, and does it fade out as one moves inward? Chances are you are dealing with inflow enhancement rather than thrombus.
Is there any evidence of phase artifacts (ghosting) adjacent to the vessel? (You may have to re-window the image and look in the air outside the patient to see it). If you do see ghosting, some flow must be present.
Does the area in question get brighter with gadolinium? Although gadolinium may diffuse into a clot, seeing a significantly brighter signal postcontrast supports the diagnosis of vascular patency. However, since tumor thrombi may enhance vividly with gadolinium, contrast enhancement will not aid much in the differential diagnosis in this scenario.
If the patient is still in the scanner at the time the questionable venous abnormality is noted a quick 2D phase-contrast MR venogram may be with a low velocity-encoding (VENC) gradient (e.g., 20 cm/sec). Slow flow will often become immediately apparent when this technique is used. Very slow flow may still be missed, however.
Another simple technique is to apply a presaturation band upstream from the site of suspected thrombosis. The signal from thrombus will be unaffected by this maneuver; flow signal will be reduced or eliminated.
Try repeating the T1- or T2-weighted images using a different plane of section than in the original. Slow flow may change its appearance, but thrombus will not.
Finally, consider repeating the sequences with and without gradient-moment nulling. Flow may change in appearance, thrombus will not.
If these techniques all fail, you may need to equivocate and recommend an additional MR, CT, or Doppler study to resolve the issue. With careful observations and employing the techniques above, this should only occasionally be necessary.
References
Idbaih A, Boukobza M, Crassard I, et al. MRI of clot in cerebral venous thrombosis: high diagnostic value of susceptibility-weighted images. Stroke 2006; 37:991-995.
Provenzale JM, Kranz PG. Dural sinus thrombosis: sources of error in image interpretation. AJR Am J Roentgenol 2011;198:23-31.
Spritzer CE, Arata MA, Freed KS. Isolated pelvic deep venous thrombosis: relative frequency as detected with MR imaging. Radiology 2001; 219:521-525.
Idbaih A, Boukobza M, Crassard I, et al. MRI of clot in cerebral venous thrombosis: high diagnostic value of susceptibility-weighted images. Stroke 2006; 37:991-995.
Provenzale JM, Kranz PG. Dural sinus thrombosis: sources of error in image interpretation. AJR Am J Roentgenol 2011;198:23-31.
Spritzer CE, Arata MA, Freed KS. Isolated pelvic deep venous thrombosis: relative frequency as detected with MR imaging. Radiology 2001; 219:521-525.
Related Questions
How can you predict whether a certain vessel will be bright or dark on an MR image?
How can you predict whether a certain vessel will be bright or dark on an MR image?