Ventricular Function
How is ejection fraction computed using cine MRI?
|
|
|
In addition to the visual inspection of cardiac wall motion and thickening on cine studies, quantitative analysis of global ventricular function is also routinely performed at most centers. After downloading data to an independent workstation, technologists trace the inner margins of the myocardium throughout the cardiac cycle. Semiautomated software now exists to assist with this process, but must always be checked by a human for accuracy. The outer myocardial borders may also be traced. The patient's weight and height are entered, allowing normalization of calculated functional parameters to a standard body surface area (BSA) of 1.8 m².
|
Automated ventricular function contours on short axis cine (Courtesy Siemens)
|
A typical left ventricular (LV) function study begins with single-slice, TrueFISP/balanced SSFP cine images in 2-chamber, 3-chamber, and 4-chamber views. For most cooperative patients without significant arrhythmias these can each be obtained using retrospective gating in a single breath-hold.
The core LV function sequence comes next — a short-axis cine of 8-12 slices perpendicular to the long axis of the LV spanning from the mitral valve to the apex throughout the cardiac cycle. These are obtained in multiple breath-holds with retrospective gating. The field-of-view (FOV) should be rotated to avoid wrap-around artifact.
Total left ventricular (LV) volumes are calculated by multiplying the cross-sectional areas in each short-axis slice by the slice thickness plus inter-slice gap (Simpson's rule). Global ventricular functional parameters generated by this process include
- End diastolic volume (EDV) = largest size of ventricular cavity during diastole (relaxation)
- End systolic volume (ESV) = smallest size of ventricular cavity during contraction (systole)
- Stroke volume (SV) = EDV−ESV = volume of blood displaced in 1 heart beat
- Ejection fraction (EF) = SV/EDV = % of blood displaced in 1 heart beat
- Cardiac output (CO) = SV x heart rate = total volume of blood displaced in 1 minute
- Cardiac index (CI) = CO/BSA = cardiac output normalized to body surface area
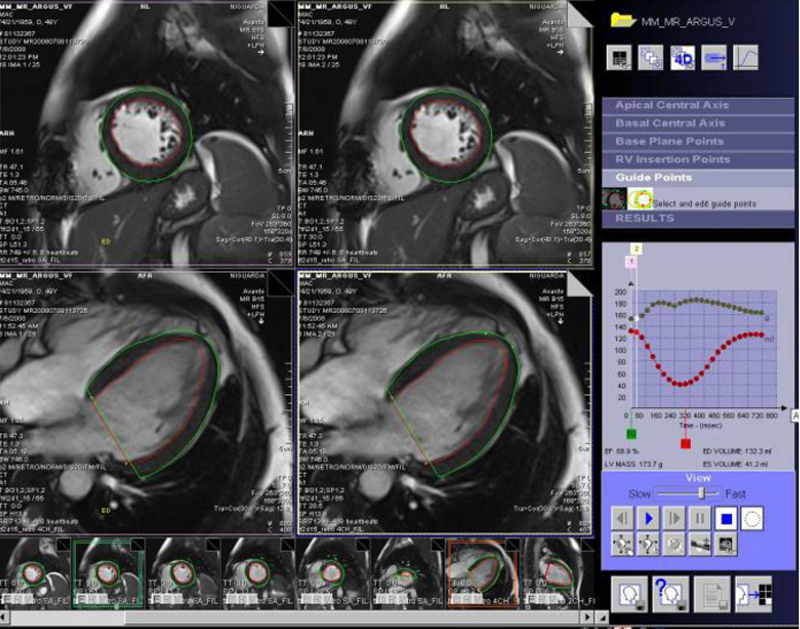
Semi-automated ventricular function analysis is available from most MR vendors and independent companies, as in this example from the Siemens Argus system.
Only LV volumes are usually calculated routinely, but the method can be applied to the right ventricle (RV) as well. Clinical scenarios requiring RV measurements include evaluation of patients with congenital heart disease, pulmonary hypertension, and arrhythmogenic right ventricular cardiomyopathy (ARVC). RV function may be difficult to assess by echocardiography due to is location directly beneath the sternum.
A typical RV function study begins with single-slice, retrospectively-gated vertical long-axis and RV outflow tract cine's. The core measurement sequence is a stack of 8-12 transverse images covering the entire RV and outflow tract.
Cardiac MR is now generally considered the "gold standard" for clinical measurement of both LV and RV function, superior to echocardiography, nuclear, and catheter ventriculography. Multiple studies in humans and animals have documented that functional parameters obtained by MRI have high reproducibility, accuracy, and low intraobserver and interobserver variability.
References
Flett A, Moon J. LV normal volumes calculator. (Requires MS-Excel. Table of normal LV ranges and interactive calculator from London Heart Hospital. Password is 'CMR' to change spreadsheet).
Kawel-Boehm N, Maceira A, Valsangiacomo-Buechel ER, et al. Normal values for cardiovascular magnetic resonance in adults and children. J Cardiovasc Magn Reson 2015; 17:29.
Maceira AM, Prasad SK, Khan M, Pennell DJ. Normalized left ventricular systolic and diastolic function by steady state free precession cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2006; 8:417-426.
Siemens. SCMR Recommended Cardiac MRI Protocols, 2013. Available from this link at Siemens Medical. (Details of LV and RV protocols can be found on pages 8-11).
Walsh TF, Hundley WG. Assessment of ventricular function with cardiovascular magnetic resonance. Cardiol Clin 2007; 25:15-33.
Flett A, Moon J. LV normal volumes calculator. (Requires MS-Excel. Table of normal LV ranges and interactive calculator from London Heart Hospital. Password is 'CMR' to change spreadsheet).
Kawel-Boehm N, Maceira A, Valsangiacomo-Buechel ER, et al. Normal values for cardiovascular magnetic resonance in adults and children. J Cardiovasc Magn Reson 2015; 17:29.
Maceira AM, Prasad SK, Khan M, Pennell DJ. Normalized left ventricular systolic and diastolic function by steady state free precession cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2006; 8:417-426.
Siemens. SCMR Recommended Cardiac MRI Protocols, 2013. Available from this link at Siemens Medical. (Details of LV and RV protocols can be found on pages 8-11).
Walsh TF, Hundley WG. Assessment of ventricular function with cardiovascular magnetic resonance. Cardiol Clin 2007; 25:15-33.
Related Questions
How do they make those movies of the beating heart?
How do they make those movies of the beating heart?