Thermal InjuriesHow do burns occur in MRI?
|
|
Thermal/electrical burns account for nearly two-thirds of clinically significant patient injuries in MRI. Most occur in the upper extremities or torso. Common causes are include: contact with a conductive object (e.g. RF coil, EKG pads/leads, clothing); contact with the wall of the scanner bore; and direct skin-to-skin contact.
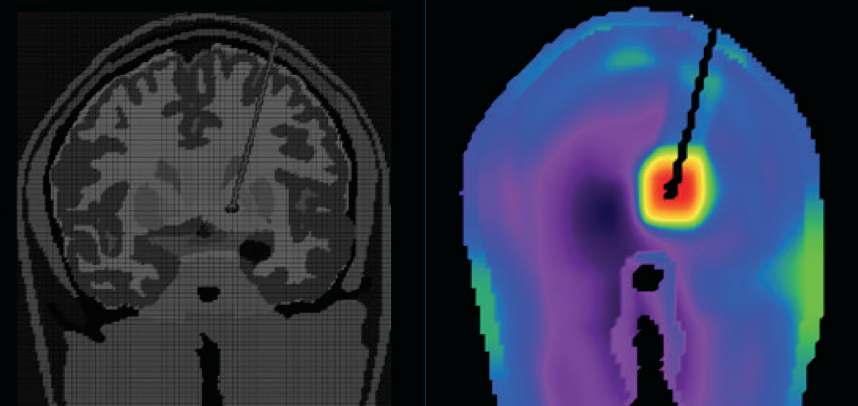 SAR "hot-spot" due to antenna effect at the tip of a deep brain stimulator.
SAR "hot-spot" due to antenna effect at the tip of a deep brain stimulator. (From Iacono et al under CC BY)
Three physical mechanisms underlying RF-induced thermal injury are recognized:
- Inductive heating. According to Faraday's Law, a changing magnetic field generates electrical currents, called eddy currents, in conductive materials. The human body is a reasonable conductor (owing to the presence ions in extracellular in intracellular fluids), and, of course, metallic foreign materials are excellent conductors. When electric currents are channeled into a small area of high resistance (such as a metal-skin interface), heat is generated that may result in burns.
- Heating of a resonant loop. Certain electrical circuits are known to resonantly absorb and release energy at a specific frequency if they form a loop that contains both capacitance and inductance elements. For example, a coiled wire lying on a patient's stomach might contribute inductance, while the skin-metal interface at radiofrequencies becomes capacitive. Although a relatively uncommon situation, resonant loops may generate the highest level of inductive heating with burns possible.
- Antenna effect. Wires and elongated conductive objects can act like antennas, capturing electromagnetic waves to extract power from them. Antennas produce standing-wave patterns of voltage and current that are concentrated near their tips, maximal when their length is one-half of the RF wavelength. For MRI, therefore, wires measuring about 26 cm at 1.5T or 13 cm at 3.0T are the most likely to create heating problems.
Surprisingly, many patients do not even know they are being burned and may only notice nothing or only minor pain or redness immediately after the scan. (The best theory for this is that the bulk of the initial injury has begun in the subcutaneous fat which lacks pain sensors.) It is not rare for patients to report blistering or increased redness and pain more than 24 hours after imaging.
Below are examples of various thermal/electrical burns, most of which could have been prevented with proper screening and patient management.

Thermal injury surrounding a large tattoo. Black pigments in tattoos are typically based upon iron oxide. See Advanced Discussion for more comments about tattoo safety.
(Courtesy Moriel NessAiver, simplyphysics.com) |

Skin-to-skin contact conductive loop ("kissing") burns on the hand and thigh (from Vister et al under CC BY)
|
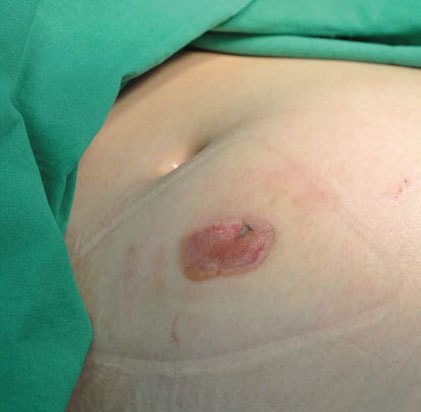
Burn where this patient's protuberant abdomen contacted the inner magnet bore during scanning. (from Lee under CC-BY)
|

Burn from an EKG pad left in place during MRI scanning.
|

Blisters developing along leg of patient wearing jogging pants containing thin metal fibers. (from Takue under CC-BY)
|

Linear burn along path of a cable touching the patient's abdomen (from Othman under CC-BY)
|

Full thickness finger burn from a pulse oximeter (from Sung et al under CC BY)
|
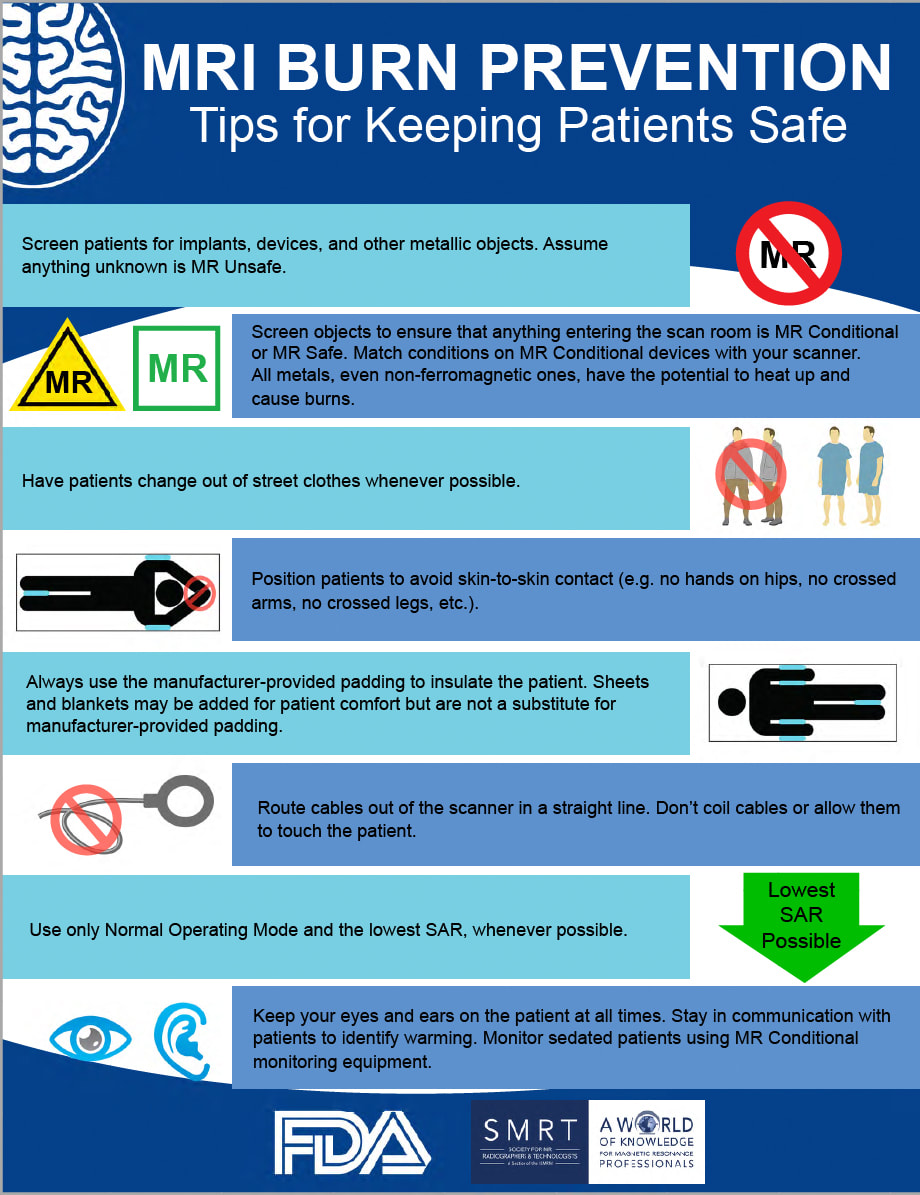
FDA/SMRT-sponsored safety poster available for MRI centers.
See Advanced Discussion for additional comments and details about these.
See Advanced Discussion for additional comments and details about these.
Additional Comments about Burns and MR Safety
Tattoos. The first degree burn associated with the dragon tattoo pictured above is a distinctly rare phenomenon. Today something like 20% of people in Europe and America have at least one tattoo, so the incidence of a severe reaction is extremely small. We therefore scan everyone with tattoos, but do warn each patient to be aware of any burning or discomfort during the scan.
Cosmetic tattoos (such as permanent eyeliner) also carry some risk, but because of their small size will seldom cause a problem. Reported cases include transient eyelid swelling, itching, and the like with no lasting sequela.
Clothing. Various sportswear and underwear are now sometimes impregnated with invisible metallic microfibers that are undetectable to the eye. Supposedly these fibers (often silver impregnated) have an antimicrobial effect. This is just one more reason that everyone getting an MRI scan should be stripped down completely (including underwear) and provided a hospital-style gown prior to MRI.
Foreign conductive/metallic objects. Scanning a patient who still has a non-MRI-compatible EKG pad, pulse oximeter, on the like should be considered a "never event" -- an egregious medical error for which no excuse is acceptable. The situations where I have seen this occur are usually in critically ill patients who are being rushed to MRI with a whole team of health care providers urging the tech to begin scanning immediately. It is good practice never to use any sheets, blankets, bedding from the hospital floor to be placed with the patient on the MR gurney, but to provide those items from the MR inventory itself.
Touching coils. Specialized MR foam padding should be used (not sheets or towels) to prevent patients from touching the walls of the scanner or the local coils. This may be difficult in very large patients but must be done.
Avoiding skin-to-skin contact. The "kissing burns" pictured above are what can happen if this rule is not observed. Typical scenarios include crossing the legs or holding ones hands.
Wires and cables. Of course, skin contact must be avoided by padding and positioning. The wires should not be allowed to cross. They should be run down the center of the MR system out between the patient's legs (not along the side of the system close to the RF coil). If more than one wire is exiting, try to leave a little space between them (to prevent capacitive coupling).
Silver-containing wound dressings. A single report to the ECRI Institute in 2007 described pain occurring in the stump of an amputee covered with a silver-containing dressing. The exact nature of this pain was never fully delineated, although MR-induced eddy current heating from silver ions was strongly suggested as the cause. To my knowledge, no other similar cases have been reported, and there are now several experimental papers that have shown no heating in a variety of silver-containing dressings.
Several companies specifically require removal of their silver-containing dressings if within the main RF/imaged field-of-view. These dressings include the Acticoat 7 (Smith and Nephew), Procellera (Vomaris), and the Silver Stump Shrinker (Juzo). Other than these, I do not recommend removal of such dressings routinely for safety reasons, but do warn the patient to be aware of any discomfort in the region of the dressing if the dressing is within the imaged field of view. Note that the silver may produce a mild local susceptibility artifact that might interfere with diagnosis, so the dressing might need to be removed and body part cleaned of silver residue for that reason.
Transdermal medication patches. Some transdermal medication patches have an aluminum or other metallic backing resulting in RF-induced cutaneous second-degree burns in a few patients. If a metal-backed patch is encountered on routine screening, the patient's physician should be contacted to see if it can be removed temporarily for MR imaging. Common metal-backed patches in this category include Androderm, Transderm-Nitro, Deponit, Nicoderm, Nicotrol, Catpres-TTS, Habitrol, TransDerm Scop (and certain other scopolomine patches). Note that if the patch is not in the region of the transmit RF-coil there is no danger. Also, non-metal-backed patches are of no concern.
Electronic patches. Many of these are for pain relief or physiologic monitoring, containing batteries and electronic components. All considered MR Unsafe and must be removed prior to imaging. These include Aleve Direct Therapy, Icy Hot Smart Relief TENS Therapy (and similar TENS units), ActiPatch, Vital Sense Dermal Patch, SCRAM alcohol monitoring system, Neulasta OnPro, and the Xio XT Patch (actually a cutaneous cardiac monitor).
Tattoos. The first degree burn associated with the dragon tattoo pictured above is a distinctly rare phenomenon. Today something like 20% of people in Europe and America have at least one tattoo, so the incidence of a severe reaction is extremely small. We therefore scan everyone with tattoos, but do warn each patient to be aware of any burning or discomfort during the scan.
Cosmetic tattoos (such as permanent eyeliner) also carry some risk, but because of their small size will seldom cause a problem. Reported cases include transient eyelid swelling, itching, and the like with no lasting sequela.
Clothing. Various sportswear and underwear are now sometimes impregnated with invisible metallic microfibers that are undetectable to the eye. Supposedly these fibers (often silver impregnated) have an antimicrobial effect. This is just one more reason that everyone getting an MRI scan should be stripped down completely (including underwear) and provided a hospital-style gown prior to MRI.
Foreign conductive/metallic objects. Scanning a patient who still has a non-MRI-compatible EKG pad, pulse oximeter, on the like should be considered a "never event" -- an egregious medical error for which no excuse is acceptable. The situations where I have seen this occur are usually in critically ill patients who are being rushed to MRI with a whole team of health care providers urging the tech to begin scanning immediately. It is good practice never to use any sheets, blankets, bedding from the hospital floor to be placed with the patient on the MR gurney, but to provide those items from the MR inventory itself.
Touching coils. Specialized MR foam padding should be used (not sheets or towels) to prevent patients from touching the walls of the scanner or the local coils. This may be difficult in very large patients but must be done.
Avoiding skin-to-skin contact. The "kissing burns" pictured above are what can happen if this rule is not observed. Typical scenarios include crossing the legs or holding ones hands.
Wires and cables. Of course, skin contact must be avoided by padding and positioning. The wires should not be allowed to cross. They should be run down the center of the MR system out between the patient's legs (not along the side of the system close to the RF coil). If more than one wire is exiting, try to leave a little space between them (to prevent capacitive coupling).
Silver-containing wound dressings. A single report to the ECRI Institute in 2007 described pain occurring in the stump of an amputee covered with a silver-containing dressing. The exact nature of this pain was never fully delineated, although MR-induced eddy current heating from silver ions was strongly suggested as the cause. To my knowledge, no other similar cases have been reported, and there are now several experimental papers that have shown no heating in a variety of silver-containing dressings.
Several companies specifically require removal of their silver-containing dressings if within the main RF/imaged field-of-view. These dressings include the Acticoat 7 (Smith and Nephew), Procellera (Vomaris), and the Silver Stump Shrinker (Juzo). Other than these, I do not recommend removal of such dressings routinely for safety reasons, but do warn the patient to be aware of any discomfort in the region of the dressing if the dressing is within the imaged field of view. Note that the silver may produce a mild local susceptibility artifact that might interfere with diagnosis, so the dressing might need to be removed and body part cleaned of silver residue for that reason.
Transdermal medication patches. Some transdermal medication patches have an aluminum or other metallic backing resulting in RF-induced cutaneous second-degree burns in a few patients. If a metal-backed patch is encountered on routine screening, the patient's physician should be contacted to see if it can be removed temporarily for MR imaging. Common metal-backed patches in this category include Androderm, Transderm-Nitro, Deponit, Nicoderm, Nicotrol, Catpres-TTS, Habitrol, TransDerm Scop (and certain other scopolomine patches). Note that if the patch is not in the region of the transmit RF-coil there is no danger. Also, non-metal-backed patches are of no concern.
Electronic patches. Many of these are for pain relief or physiologic monitoring, containing batteries and electronic components. All considered MR Unsafe and must be removed prior to imaging. These include Aleve Direct Therapy, Icy Hot Smart Relief TENS Therapy (and similar TENS units), ActiPatch, Vital Sense Dermal Patch, SCRAM alcohol monitoring system, Neulasta OnPro, and the Xio XT Patch (actually a cutaneous cardiac monitor).
References
Bailey JK, Sammet S, Overocker J, et al. MRI compatibility of silver based wound dressings. Burns 2018; 44:1940-1946. [DOI LINK]
Delfino JG, Krainak DM, Flesher SA. MRI-related FDA adverse events reports: a 10-yr review. Med Phys 2019; 46:5562-5571. [DOI LInk] (summary of 906 injuries from 2008-2017)
Dempsey MF, Condon B, Hadley DM. Investigation of the factors responsible for burns during MRI. J Magn Reson Imaging 2001; 13:627-631. [DOI Link]
Hardy PT, Weil KM. A review of thermal MR injuries. Radiol Technol 2010;81:606-9. (summary of thermal injuries from 1997-2009).
Iacono MI, Makris N, Mainardi L, et al. MRI-based multi scale model for electromagnetic analysis in the human head with implanted DBS. Comput Math Methods Med 2013; 2013:694171. [DOI Link]
Lee C-M, Kang B-K, Song S-Y, et al. MRI induced second-degree burn in a patient with extremely large uterine leiomyomas: a case report. J Korean Soc Radiol 2015; 73:424-427. [DOI Link]
Nyenhuis J, Duan L. An evaluation fo MRI safety and compatibility of a silver-impregnated antimicrobial wound dressing. J am Coll Radiol 2009; 6:500-505. [DOI LINK]
Othman D, Abdel-Rehim S, O’Boyle C. MRI-induced burns from ECG leads: thermal or electrical burns? Ann Burns Trauma 2017; 1:104.
Sung SJ, Park YS, Cho JY. Full thickness burn on the finger due to pulse oximetry during magnetic resonance imaging in a conscious patient. Arch Plast Surg 2016: 43:612-613. [DOI Link]
Tokue H, Tokue A, Tsushima Y. Unexpected magnetic resonance imaging burn injuries from jogging pants. Radiology Case Reports 2019; 14:1348–135. [DOI Link]
[Vister J, van Erling L, Steens SC, Meljer FJA. Brandwonden tijdens een MRI-scan (“Burn during an MRI scan”). Ned Tijdschr Geneeskd 2014; 158:A7927] Dutch
Bailey JK, Sammet S, Overocker J, et al. MRI compatibility of silver based wound dressings. Burns 2018; 44:1940-1946. [DOI LINK]
Delfino JG, Krainak DM, Flesher SA. MRI-related FDA adverse events reports: a 10-yr review. Med Phys 2019; 46:5562-5571. [DOI LInk] (summary of 906 injuries from 2008-2017)
Dempsey MF, Condon B, Hadley DM. Investigation of the factors responsible for burns during MRI. J Magn Reson Imaging 2001; 13:627-631. [DOI Link]
Hardy PT, Weil KM. A review of thermal MR injuries. Radiol Technol 2010;81:606-9. (summary of thermal injuries from 1997-2009).
Iacono MI, Makris N, Mainardi L, et al. MRI-based multi scale model for electromagnetic analysis in the human head with implanted DBS. Comput Math Methods Med 2013; 2013:694171. [DOI Link]
Lee C-M, Kang B-K, Song S-Y, et al. MRI induced second-degree burn in a patient with extremely large uterine leiomyomas: a case report. J Korean Soc Radiol 2015; 73:424-427. [DOI Link]
Nyenhuis J, Duan L. An evaluation fo MRI safety and compatibility of a silver-impregnated antimicrobial wound dressing. J am Coll Radiol 2009; 6:500-505. [DOI LINK]
Othman D, Abdel-Rehim S, O’Boyle C. MRI-induced burns from ECG leads: thermal or electrical burns? Ann Burns Trauma 2017; 1:104.
Sung SJ, Park YS, Cho JY. Full thickness burn on the finger due to pulse oximetry during magnetic resonance imaging in a conscious patient. Arch Plast Surg 2016: 43:612-613. [DOI Link]
Tokue H, Tokue A, Tsushima Y. Unexpected magnetic resonance imaging burn injuries from jogging pants. Radiology Case Reports 2019; 14:1348–135. [DOI Link]
[Vister J, van Erling L, Steens SC, Meljer FJA. Brandwonden tijdens een MRI-scan (“Burn during an MRI scan”). Ned Tijdschr Geneeskd 2014; 158:A7927] Dutch