ASL Methods Overview
Can you briefly explain the difference between the various ASL methods? Which is the best?
|
|
Classification of ASL techniques
|
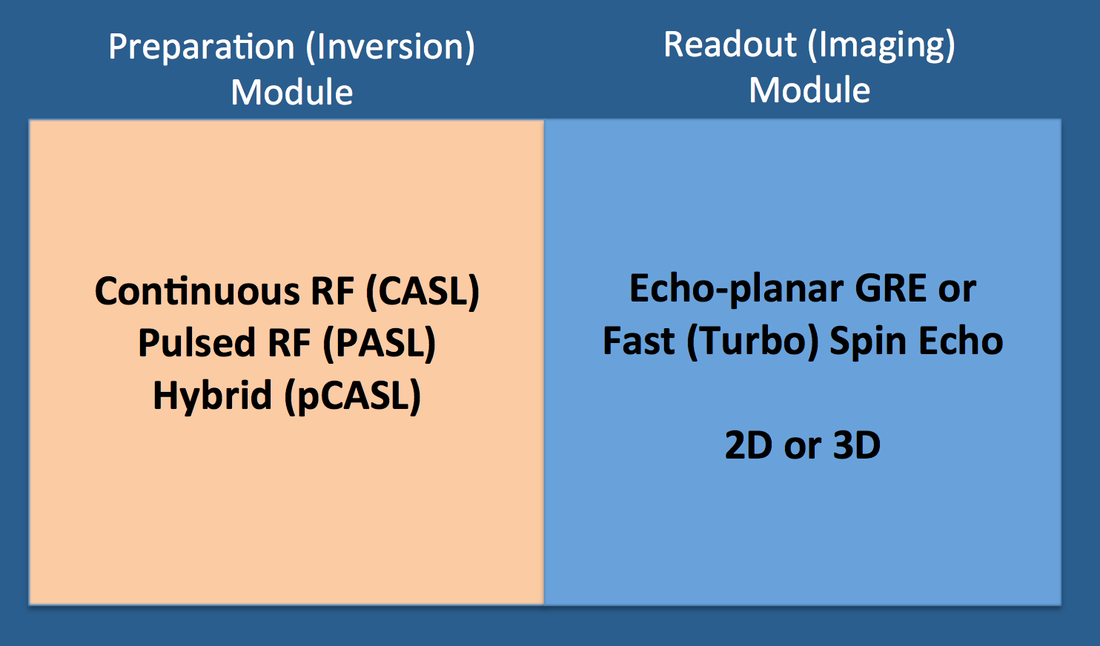
All arterial spin labeling (ASL) pulse sequences consist of two components: 1) a preparation module to magnetically label/tag flowing blood, and 2) a readout module to generate paired images of the target tissue under "control" and "tagged" conditions. ASL methods may be classified as to how each of these modules is constructed.
|
The earliest ASL techniques inverted flowing spins using continuous radiofrequency (RF) irradiation in conjunction with magnetic field gradients applied in the direction of blood flow. Known by the acronym CASL (Continuous Arterial Spin Labeling), these sequences were difficult to implement on commercial scanners and produced significant tissue heating. By the late 1990s CASL methods were largely abandoned in favor of a group of methods using pulsed irradiation, known collectively as PASL (Pulsed Arterial Spin Labeling). PASL techniques can be further divided into those that label spins asymmetrically with respect to the plane of imaging (EPISTAR, PICORE) or symmetrically (FAIR). More recently a hybrid form has been developed, pCASL (pseudo-Continuous Arterial Spin Labeling), that uses a long series of short RF-pulses together with a strong slice-selection gradient. pCASL thus combines favorable features of CASL (high signal-to-noise) with those of PASL (lower energy deposition). Today most commercially available ASL products are based on pCASL or a PASL variant.
In the earliest ASL methods readout (imaging) was confined to a single slice obtained with an echo-planar gradient echo technique. Multi-slice methods soon followed, as well as image formation using fast (turbo) spin echoes and turbo gradient spin echoes. Both multi-slice 2D and 3D methods are available.
2D image acquisition is less sensitive to head motion and is probably better than 3D for blood flow quantification. For optimal image quality, both a prescan as well as field mapping are recommended. A disadvantage of 2D methods is that more distal slices have longer labeling delays than proximal slices, resulting in slice-to-slice variations in signal due to relaxation effects.
3D methods take slightly longer than 2D methods to perform, but are easier to set up. They offer higher signal-to-noise and better spatial resolution, as well as a fixed labeling delay across all slices. At present 3D techniques are not compatible with fMRI studies as perfusion changes over short time intervals cannot be obtained. Background suppression is also generally required that reduces perfusion signal and may confound calculation of absolute blood flows.
3D methods take slightly longer than 2D methods to perform, but are easier to set up. They offer higher signal-to-noise and better spatial resolution, as well as a fixed labeling delay across all slices. At present 3D techniques are not compatible with fMRI studies as perfusion changes over short time intervals cannot be obtained. Background suppression is also generally required that reduces perfusion signal and may confound calculation of absolute blood flows.
Technical details and more complete descriptions of the major ASL sequences are covered in the next several Q&A's.
References
Borogovac A, Asllani I. Arterial spin labeling (ASL) fMRI: advantages, theoretical constrains and experimental challenges in neurosciences. Int J Biomed Imaging 2012; Article ID 818456:1-13.
Diebler AR, Pollock JM, Kraft RA, et al. Arterial spin-labeling in routine clinical practice, Part 1: techniques and artifacts. AJNR Am J Neuroradiol 2008; 29:1228-1234.
Essig M, Shiroishi MS, Nguyen TB, et al. Perfusion MRI: the five most frequently asked technical questions. AJR Am J Roentgenol 2013; 200:24-34.
Ferré J-C, Bannier E, Raoult H, et al. Arterial spin labeling (ASL) perfusion: techniques and clinical use. Diagn Interv Radiol 2013; 94:1211-1223
Jahng G-H, Li K-L, Ostergaard l, Calamante F. Perfusion magnetic resonance imaging: a comprehensive update on principles and techniques. Korean J Radiol 2014; 15:554-577. (good recent review).
Knutsson L, Xu J, Ahlgren A, van Zijl PCM. CEST, ASL and magnetization transfer contrast: how similar pulse sequences detect different phenomena. Magn Reson Med 2018; 1320-1340.
McGehee BE, Pollock JM, Maldjian JA. Brain perfusion imaging: how does it work and what should I use? J Magn Reson Imaging 2012; 36:1257-1272.
Wong EC, Cronin M, Wu W-C, et al. Velocity-selective arterial spin labeling. Magn Reson Med 2006; 55:1334-1341.
Borogovac A, Asllani I. Arterial spin labeling (ASL) fMRI: advantages, theoretical constrains and experimental challenges in neurosciences. Int J Biomed Imaging 2012; Article ID 818456:1-13.
Diebler AR, Pollock JM, Kraft RA, et al. Arterial spin-labeling in routine clinical practice, Part 1: techniques and artifacts. AJNR Am J Neuroradiol 2008; 29:1228-1234.
Essig M, Shiroishi MS, Nguyen TB, et al. Perfusion MRI: the five most frequently asked technical questions. AJR Am J Roentgenol 2013; 200:24-34.
Ferré J-C, Bannier E, Raoult H, et al. Arterial spin labeling (ASL) perfusion: techniques and clinical use. Diagn Interv Radiol 2013; 94:1211-1223
Jahng G-H, Li K-L, Ostergaard l, Calamante F. Perfusion magnetic resonance imaging: a comprehensive update on principles and techniques. Korean J Radiol 2014; 15:554-577. (good recent review).
Knutsson L, Xu J, Ahlgren A, van Zijl PCM. CEST, ASL and magnetization transfer contrast: how similar pulse sequences detect different phenomena. Magn Reson Med 2018; 1320-1340.
McGehee BE, Pollock JM, Maldjian JA. Brain perfusion imaging: how does it work and what should I use? J Magn Reson Imaging 2012; 36:1257-1272.
Wong EC, Cronin M, Wu W-C, et al. Velocity-selective arterial spin labeling. Magn Reson Med 2006; 55:1334-1341.
Related Questions
What is PASL and how does it differ from CASL?
What is pCASL and how does it differ from CASL and PASL?
What is PASL and how does it differ from CASL?
What is pCASL and how does it differ from CASL and PASL?