MRA Methods
How do you create an MR angiogram?
|
|
MRA methods can be divided into two broad categories depending on whether they produce dark blood or bright blood. Bright blood techniques are further subdivided according to whether they are performed with or without gadolinium contrast.
Classification of MRA techniques
Abbreviations: FSE = fast spin echo, IR = inversion recovery, SWI = susceptibility weighted imaging, TOF = time-of-flight, PC = phase contrast, SSFP = steady-state free precession, ASL = arterial spin labelling |
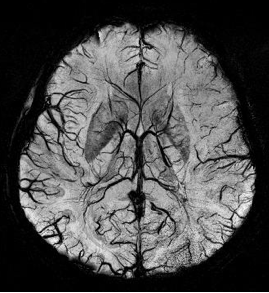
Dark blood MRA (SWI)
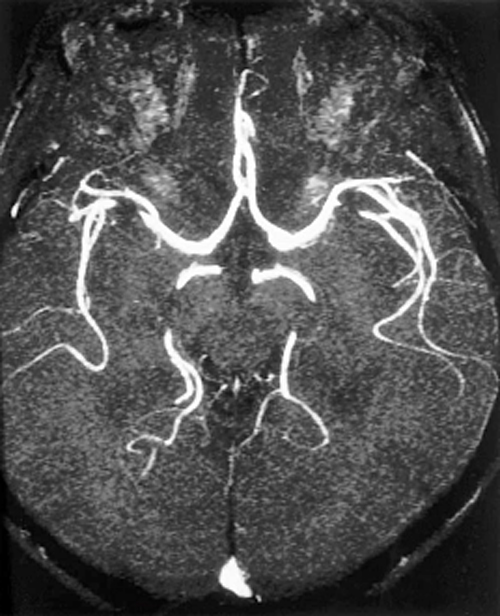
Bright blood MRA (TOF)
|
Dark Blood MRA
Dark ("black") blood MRA techniques suppress signal from flowing blood while maintaining high signal in the surrounding stationary tissues, thus rendering the vessels black. The dark blood effect may be achieved by accentuating flow-related dephasing or exploiting the T1 and T2 properties of blood. Flow saturation pulses can also be used with any of these techniques to further to suppress intravascular signal.
- Fast Spin Echo (FSE) Black Blood MRA. FSE black blood techniques depend primarily on the phenomenon of flow-related signal loss (also known as the "washout" effect), with additional contributions from spin-dephasing, all described in a prior Q&A. The classic vascular "flow void" seen on routine MR imaging is a crude form of black-blood MRA that derives from these same phenomena.
- Inversion Recovery (IR) Black Blood MRA. Single, double, or even triple 180°-inversion pulses may be used to suppress the signal from blood and other tissues (such as fat or myocardium) based on their respective T1 values. At 1.5T inversion times (TI) of 500-700 msec are used to null the signal from blood. Black blood IR methods are most commonly used for cardiac and vessel wall imaging.
- Susceptibility-weighted (SW) Black Blood MRA. Although more commonly used for the detection of calcification and hemorrhage, SW imaging was originally developed as a black blood venography technique. The paramagnetic effects of deoxyhemoglobin (present in high concentrations in venous blood) significantly shortens T2 and T2* in the vicinity of veins. 3D gradient echo sequences with long TE values are used to accentuate T2* dephasing, and the images displayed with a minimum intensity projection algorithm.
Bright Blood MRA
Contrast-enhanced MRA methods require rapid injection of a gadolinium-based agent through a large peripheral vein. Paramagnetic contrast shortens the relaxation times of blood, rendering vessels bright on T1-weighted images. After circulating through the heart, a set of images is rapidly acquired through the area of interest. The signal from background tissue is often removed by a subtraction technique. Like its close cousin, CT angiography, contrast-enhanced MRA derives its heightened intravascular signal purely from the presence of contrast material and does not depend on MR-based flow phenomena.
Non-contrast MRA methods, by comparison, are based entirely on the MR properties of flowing blood, including its intrinsic relaxation times, time-of-flight (TOF), and spin-phase effects. Several variations are possible:
- Time-of-Flight (TOF) MRA. These methods exploit the inflow-enhancement effect described in a prior Q&A. Here, fully magnetized blood emits a high signal when it flows into a volume of stationary tissue that has been magnetically saturated by rapidly repeated RF-pulses. TOF MRA is among the oldest and most popular methods of non-contrast MRA
- Phase-contrast (PC) MRA. Phase-contrast techniques exploit spin-phase effects that have been more completely discussed in a prior Q&A. As protons flow through a magnetic field gradient, they gain or lose phase compared to stationary background tissue. This phase change may be translated into an angiographic image. Because phase shift is directly related to blood flow, PC methods are widely used to measure vascular and CSF flow.
- Steady-state Free Precession (SSFP) MRA. Balanced SSFP techniques like TrueFISP are emerging as important methods for noncontrast MRA of the chest, abdomen, and pelvis. High intravascular signal results from the intrinsically large T2/T1 ratio of blood compared to that of solid tissues.
- Fast Spin Echo (FSE) MRA. This method obtains cardiac-gated FSE images in systole and diastole. During diastole, the signal in both arteries and veins is high reflecting the long T2 of blood. During systole, venous signal remains high but arterial signal drops due to flow-related signal loss. Subtraction of the systolic from the diastolic images results in a pure arterial image.
- Arterial Spin Labeling (ASL) MRA. In ASL methods upstream spins (which subsequently flow into the imaged volume) are first "tagged" with a 180°-inversion pulse. Background tissue is suppressed either by a subtraction method requiring two acquisitions or by applying a spatially nonselective pulse to the imaged volume in a single acquisition. ASL techniques can be combined with SSFP or FSE methods for an enhanced effect.
Each of these basic MRA methods will be described in detail in subsequent Q&A's. Many variations and combinations are possible.
References
Hartung MP, Grist TM, François CJ. Magnetic resonance angiography: current status and future directions. J Cardiovasc Magn Reson 2011; 13:19-30.
Miyazaki M, Lee VS. Nonenhanced MR angiography. Radiology 2008;248:20-43.
Saloner D. An introduction to MR angiography. Radiographics 1995;15:453-465. (Older review; good discussion of TOF and PC MRA)
Wheaton AJ, Miyazaki M. Non-contrast enhanced MR angiography: physical principles. J Magn Reson Imaging 2012; 36:286-304.
Hartung MP, Grist TM, François CJ. Magnetic resonance angiography: current status and future directions. J Cardiovasc Magn Reson 2011; 13:19-30.
Miyazaki M, Lee VS. Nonenhanced MR angiography. Radiology 2008;248:20-43.
Saloner D. An introduction to MR angiography. Radiographics 1995;15:453-465. (Older review; good discussion of TOF and PC MRA)
Wheaton AJ, Miyazaki M. Non-contrast enhanced MR angiography: physical principles. J Magn Reson Imaging 2012; 36:286-304.
Related Questions
What are time-of-flight effects?
What are spin-phase effects?
Why would you want to choose dark blood over bright blood for MRA? Can't you just invert the bright blood image on a monitor and get the same effect?
What are time-of-flight effects?
What are spin-phase effects?
Why would you want to choose dark blood over bright blood for MRA? Can't you just invert the bright blood image on a monitor and get the same effect?