MR Safety: Bullets and ShrapnelHow do you handle a patient who has a retained bullet, pellet, or metallic shrapnel?
|
|
In the United States approximately 100,000 patients per year present to emergency rooms with gunshot wounds. When these patients require an MRI (either acutely or years later), the presence of retained bullet fragments and shrapnel pose important safety concerns that must be addressed. Firearm projectiles are commonly divided into three groups:
- BB's and pellets are small projectiles fired using an air- or spring-loaded gun. BB's are spherical and made of ferromagnetic steel coated with copper or zinc (to resist corrosion). Pellets typically have a mushroom shape (for aerodynamics) and are predominantly made of lead or tin-based alloys, but occasionally copper or steel.
|

Steel-containing jacketed MR bullets (shell casing containing gunpowder has been removed)
|


Regardless of their metallic composition, bullets, shot, and bits of shrapnel do not produce significant RF-heating due to their overall small dimensions. Projectiles composed of only non-ferromagnetic materials (e.g., lead, copper, brass, or zinc) neither undergo heating nor significant translational or or rotational forces. They should thus be considered OK to scan under any conditions. The primary safety concern is for projectiles containing ferromagnetic steel which can move significantly when placed in a strong external magnetic field.
My basic approach to screening patients with gunshot injuries involves assessing the diagnostic benefit of MRI vs the risk. The benefit analysis depends on the particular clinical scenario and the likelihood that an alternative technique (such as CT or US) could answer the diagnostic question. My risk analysis, described below, is based upon the a priori probability that the projectile is ferromagnetic, as well as its precise anatomic location and time since injury.
Assessing the Probability of Ferromagnetism
- All bullets and shrapnel acquired in military service or overseas should be considered ferromagnetic unless proven otherwise.
- All BB's and pellets should be considered ferromagnetic.
- All shotgun pellets should be considered ferromagnetic, although about half are not. Pellets that distort into multiple irregular (non-rounded) shapes are more likely to be made of lead.
- Bullets from pistols and handguns in the USA virtually never contain steel, as their manufacture and sale (but not possession) has been a federal crime since the attempted assassination of President Reagan in 1986.
- Bullets from domestic handguns implanted more than 25 years ago should be considered ferromagnetic out of extra caution, although the probability is low.
- Armor-piercing steel-jacketed and steel-cored bullets can and are legally sold for use in rifles in the USA and elsewhere. Being so powerful/penetrating they would likely pass straight through a person unless stopped by a large bone. Although the probability is small that a domestic rifle bullet found on screening would be ferromagnetic, it should assumed to be so out of caution.
- Steel jacketed ammunition represents a large amount of "non-defense" ammunition (i.e., that meant for target practice)
- "Defense" ammunition, synonymous with hollow point or expanding ammunition, never contains a steel jacket as it does not aid in projectile expansion and fragmentation
- Some superficially located ferromagnetic pellets and bullets may be positively identified by a hand-held ferromagnetic metal detector; but a negative reading should be considered inconclusive.
- Some investigators have proposed using expanded range dynamic CT or dual-energy CT to determine bullet composition, but to date the results have been variable.
|
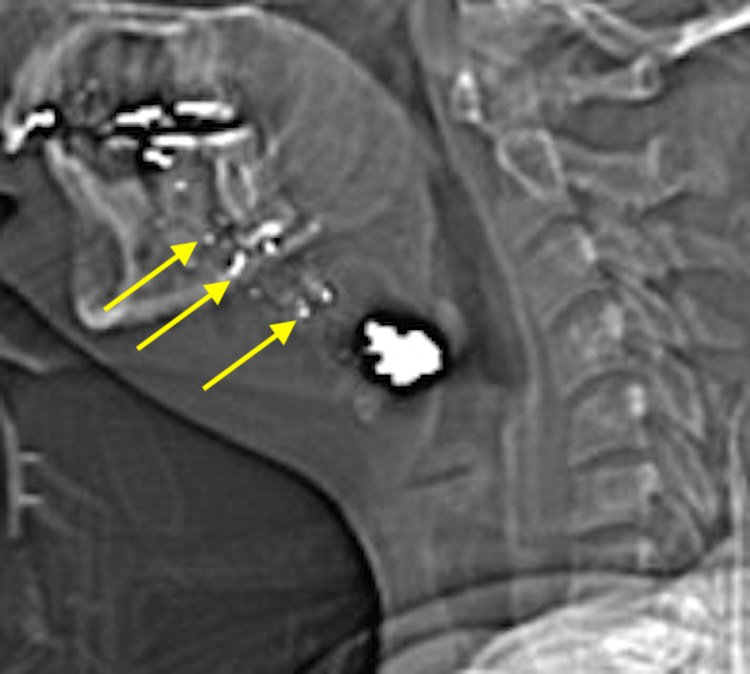
Deformed bullet in the neck with a debris trail (arrows) suggesting this is not a steel-containing projectile.
|
Assessing Risk of Injury Based on Projectile Location and Age
If a projectile does contain steel and is subjected to magnetic displacement forces, the risk to the patient depends on its precise anatomic location and how long ago implantation occurred. In vitro experiments with ferromagnetic bullets placed in gelatin or animal organs have been shown to move by up to 10 cm at 1.5T and 3.0T. So a recently acquired ferromagnetic bullet embedded in relatively "soft" soft tissues (e.g., brain, liver, spleen, lung) or in fat near major vessels, nerves, or solid organs carries a high risk of movement and possible injury. Conversely, ferromagnetic projectiles embedded in "tougher" solid tissues like bone, tendons, or skeletal muscle are much less likely to move enough to cause significant damage. The length of time since implantation should also be considered. Projectiles embedded months or years before are more likely to be restrained by a capsule of scar tissue, limiting their motion and potential damage.
Non-Firearm Shrapnel
The same rules above generally apply to non-firearm derived shrapnel, such as fragments from bombs, industrial accidents, and metal-working. Out of an abundance of safety, all such shrapnel should be considered ferromagnetic until proven otherwise. Shrapnel pieces may be larger and longer than bullets, and may therefore experience more magnetic displacement/torque and be at risk for RF-heating. The edge characteristics of the shrapnel should also be considered, with sharp edges near critical anatomic structures an additional risk.
References
Bollinger SA, Thali MJ, Gascho D, et al. Movement of steel-jacketed projectiles in biological tissue in the magnetic field of a 3-T magnetic resonance unit. In J Legal Med 2017; 131:1363-1368. [DOI LINK]
Dedini RD, Karacozoff AM, Shellock FG, et al. MRI issues for ballistic objects: information obtained at 1.5-, 3- and 7-Tesla. Spine J 2013; 13:815-822. [DOI LINK]
Ditkofsky N, Colak E, Kirpalani A, et al. MR imaging in the presence of ballistic debris of unknown
composition: a review of the literature and practical approach. Emerg Radiol 2020; 27:527-532. [DOI LINK]
Eshed I, Kushnir T, Shabshin N, et al. Is magnetic resonance imaging safe for patients with retained metal fragments from combat and terrorist attacks? Acta Radiol 2010;51:170–4. (They say "yes" but the examples shown are all subcutaneous and < 1 cm in size).
Fountain AJ, Corey A, Malko JA, et al. Imaging appearance of ballistic wounds predicts bullet composition: implications for MRI safety. AJR Am J Roentgenol 2021; 216:542-551. [DOI LINK]
Gascho D, Zoelch N, Richter H, et al. Identification of bullets based on their metallic components and x-ray attenuation characteristics at different energy levels on CT. AJR Am J Roentgenol 2019; 213:W105-113. [DOI LINK]
Teitelbaum G, Yee C, Van Horn D, et al. Metallic ballistic fragments: MR imaging safety and artifacts. Radiology 1990;175:855–9.
Bollinger SA, Thali MJ, Gascho D, et al. Movement of steel-jacketed projectiles in biological tissue in the magnetic field of a 3-T magnetic resonance unit. In J Legal Med 2017; 131:1363-1368. [DOI LINK]
Dedini RD, Karacozoff AM, Shellock FG, et al. MRI issues for ballistic objects: information obtained at 1.5-, 3- and 7-Tesla. Spine J 2013; 13:815-822. [DOI LINK]
Ditkofsky N, Colak E, Kirpalani A, et al. MR imaging in the presence of ballistic debris of unknown
composition: a review of the literature and practical approach. Emerg Radiol 2020; 27:527-532. [DOI LINK]
Eshed I, Kushnir T, Shabshin N, et al. Is magnetic resonance imaging safe for patients with retained metal fragments from combat and terrorist attacks? Acta Radiol 2010;51:170–4. (They say "yes" but the examples shown are all subcutaneous and < 1 cm in size).
Fountain AJ, Corey A, Malko JA, et al. Imaging appearance of ballistic wounds predicts bullet composition: implications for MRI safety. AJR Am J Roentgenol 2021; 216:542-551. [DOI LINK]
Gascho D, Zoelch N, Richter H, et al. Identification of bullets based on their metallic components and x-ray attenuation characteristics at different energy levels on CT. AJR Am J Roentgenol 2019; 213:W105-113. [DOI LINK]
Teitelbaum G, Yee C, Van Horn D, et al. Metallic ballistic fragments: MR imaging safety and artifacts. Radiology 1990;175:855–9.
Related Questions
How do you calculate the magnetic force pulling a piece of metal toward the scanner?
Should MRI facilities screen patients with metal detectors?
How do you calculate the magnetic force pulling a piece of metal toward the scanner?
Should MRI facilities screen patients with metal detectors?