Safety of Dental and Maxillofacial ImplantsMust a patient remove dentures and other oral prosthetics before MRI?
|
|
In general the vast majority of dental devices and implants can be considered "MR Safe" or MR Conditional, although relatively few have undergone rigorous testing of displacement, torque, and heating effects as specified by the American Society of Testing and Materials (ASTM) to earn these official labels. Other than a few relatively isolated instances described below, I am aware of no significant patient injuries due to scanning of any type of dental implant. Some authorities have recommended careful inspection of the non-removable, fixed dental devices prior to MRI to insure that the components are loose or dislodged, but we seldom do this in practice unless the patient reports that the device is loose.
Some metal-containing orthodontic devices (such as brace archwires, palate expanders, and functional fixed appliances) will undergo RF-heating, though at levels far below the 8ºC−10ºC heat pain threshold for oral mucosa or injury to the highly heat-sensitive periodontal ligament. They may also experience some deflection or torque in the static field that may exceed their weight, but this should not be of concern if they are securely anchored. In the absence of specific manufacturers' recommendations or published testing, it is wise to consider most metallic implants to be at least MR Conditional with patients given instructions to be attuned to the possibility of implant heating or a pulling sensation on the devices during the scan. Performing MRI in "Normal Operating Mode" and avoiding high SAR sequences wherever possible should be considered.
Devices Without Magnets
Conventional Dentures. Conventional dentures are typically made of composite resin, acrylic, or porcelain without any metal components. (Magnetic dentures are discussed below). Conventional dentures are fully safe to scan and do not need to be removed prior to MRI. If conscious sedation is to be used during the scan, however, we recommend that dentures and other easily removable oral appliances such as retainers be taken out to reduce chances of airway obstruction.
Fillings. Materials commonly used to fill dental caries include amalgam (primarily mercury/sliver, plus tin and copper), gold, porcelain, composite resins, and glass ionomer. As these substances are either diamagnetic or weakly paramagnetic, no MR safety concerns exist. (Note: A number of countries, but not the US, have banned the use of some dental amalgams because of slow mercury release. MRI exposure, especially at 7T, appears to temporarily accelerate this process).
Crowns and Bridges. Most dental crowns and bridges are made of resin, ceramic, or porcelain and are non-magnetic. A moderate number of metal or porcelain-on-metal devices also exist, most commonly composed of gold, palladium, nickel or chromium. The latter two metals are ferromagnetic, and will create a moderate local susceptibility artifact on MRI. In general we have no medical concerns in scanning a patient with metal crowns or bridges and take no special precautions. That said, one case report describes a loose metal crown being pulled off a tooth during MRI. A second case report describes the premature termination of an MR scan due to pain from apparent magnetic traction on a metal crown.
|
Braces. Traditional metal braces are consist of brackets (cemented to each tooth) and connected by arch wires. Brackets are usually made of stainless steel, while arch wires may be stainless steel, titanium, molybdinum, or nickel-containing alloys. Standard metal braces pose no safety issues, but the multiple ferromagnetic brackets often create huge susceptibility artifacts that distort images of the face and brain. On rare occasions where MRI of these areas is essential, we have asked the patient to have the braces removed before repeat imaging.
|
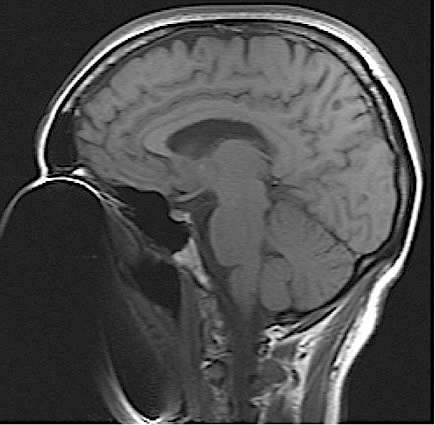
Marked susceptibility artifact due to braces
|
Devices Containing Magnets
A small number of dental, orthodontic, and maxillofacial implants contain permanent magnets. These present several additional problems compared to simple metal-containing implants.
- More artifacts. The small magnets create extremely large susceptibility artifacts, potentially obscuring not only the face but much of the head.
- Increased forces. Translational and rotational forces on the magnets are equal or greater to those from ferromagnetic metals, creating a movement risk if they are not securely attached to bone.
- Magnet damage. The magnets themselves (even those made of high coercivity Sm-Co ceramics) may undergo demagnetization or magnetization reversal in fields of 1.5T or higher, particularly when angled with respect to Bo.
In evaluating a magnet-containing device with regard to MR safety and screening, it is critical to know exactly where the magnets are located. The case of magnetic dentures provides a good example of why this is important.
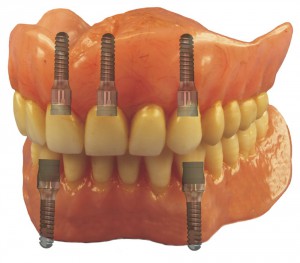 Magnetic dentures
Magnetic dentures
Magnetic Dentures. Also known as "implant overdentures", these devices are becoming increasingly popular because of their firm fit and ease of insertion and removal. The removable acrylic/ porcelain denture component has 2-4 flat permanent magnets embedded along its periphery. These match up with an equivalent set of titanium posts surgically placed in the mandible or maxilla. To the top of each post is affixed either: 1) a second small magnet with opposite polarity to its mate on the denture, or 2) with a non-magnetized but ferromagnetic abutment or "keeper". In both systems, the magnets in the denture base lock into place as they are attracted to their respective abutments or sister magnets.
The difference between these two systems is important — in one case taking out the denture removes all the magnets from the body, while in the other case it does not. It should be noted that often the retained magnetic components can be easily unscrewed by the dentist from its post or baseplate, thus allowing MRI to be safely performed.
Other Magnetic Oral and Facial Devices. Like the case of magnetic dentures, MR safety decisions must be made on a case-by-case basis depending on the nature of the implant, the location of the magnets, and the manufacturer's recommendations. The latter is primarily based upon whether the manufacturer believes the magnets from their system will be damaged by exposure to the static MRI field.
Specific examples of MR-incompatible devices based on risk of magnet dysfunction include the StecoTitanmagnetic X-,Y-, and Z-line abutments, magnetic root extrusion system, magnetic root caps, and coupled obturators (Steco-system-technik GmbH, Germany); the Sydney MagnoGlide orthodontic appliance (Macono, Australia); the Dyna implant system (Dyna Dental BV, Netherlands); and the MED osteostimulator (Magdent, Israel). Although most nasal septal button closure devices are made of plastic, one MR Unsafe model is the Blom-Singer® Nasal Septal Perforation Prosthesis (InHealth Technologies, USA) that uses paired, silicone-coated neodymium magnets. As always, please consult the manufacturer directly before making a decision about the suitability of any device for MRI.
References
Bhat VS, Shenoy KK, Premkumar P. Magnets in dentistry. Arch Med Health Sci 2013; 1:73-79. [DOI LINK]
Ceruti P, Bryant SR, Lee J-H, MacEntee MI. Magnet-retained implant-supported overdentures: review and 1-year clinical report. J Can Dent Assoc 2010; 76:a52. [LINK]
Chockattu SJ, Suryakant DB, Thakur S. Unwanted effects due to interactions between dental materials and magnetic resonance imaging: a review of the literature. Resto Dent Endod 2018; 43:e39 [DOI LINK]
Hasegawa M, Fiyata K, Abe Y, et al. 3-T MRI safety assessments of magnetic dental attachments and castable magnetic alloys. Dentomaxillofac Radiol 2015; 44:20150011. [DOI Link]
Hayashi N, Ogura A, Tsuchihashi T, et al. Magnetization and demagnetization of magnetic dental attachments in a 3-T MRI system. Radiol Phys Technol 2017; 10:294-300. [DOI LINK]
Kemper J, Priest AN, Schulze D, et al. Orthodontic springs and auxiliary appliances: assessment of magnetic field interactions associated with 1.5 T and 3 T magnetic resonance systems. Eur Radiology 2007; 17:533-540. [DOI LINK]
Mathew CA, Maller S, Maheshwaran. Interactions between magnetic resonance imaging and dental material. J Pharm Bioallied Sci 2013; 5(Suppl 1):S113-S116. [DOI LINK]
Miyata K, Hasegawa M, Abe Y, et al. Radiofrequency heating and magnetically induced displacement of dental magnetic attachments during 3.0 T MRI. Dentomaxillofac Radiol 2012; 41:66-7671. [DOI LINK]
Wilson BJ, O’hare PE, Zacariah J. Implications and considerations of dental materials in MRI: a case report and literature review. Case Reports in Dentistry 2020; Article ID 8891302 [DOI LINK]
Yilmaz S, Aiden MZ. Ex vivo mercury release from dental amalgam after 7.0-T and 1.5-T MRI. Radiology 2018; 288:799-803. [DOI link]
Bhat VS, Shenoy KK, Premkumar P. Magnets in dentistry. Arch Med Health Sci 2013; 1:73-79. [DOI LINK]
Ceruti P, Bryant SR, Lee J-H, MacEntee MI. Magnet-retained implant-supported overdentures: review and 1-year clinical report. J Can Dent Assoc 2010; 76:a52. [LINK]
Chockattu SJ, Suryakant DB, Thakur S. Unwanted effects due to interactions between dental materials and magnetic resonance imaging: a review of the literature. Resto Dent Endod 2018; 43:e39 [DOI LINK]
Hasegawa M, Fiyata K, Abe Y, et al. 3-T MRI safety assessments of magnetic dental attachments and castable magnetic alloys. Dentomaxillofac Radiol 2015; 44:20150011. [DOI Link]
Hayashi N, Ogura A, Tsuchihashi T, et al. Magnetization and demagnetization of magnetic dental attachments in a 3-T MRI system. Radiol Phys Technol 2017; 10:294-300. [DOI LINK]
Kemper J, Priest AN, Schulze D, et al. Orthodontic springs and auxiliary appliances: assessment of magnetic field interactions associated with 1.5 T and 3 T magnetic resonance systems. Eur Radiology 2007; 17:533-540. [DOI LINK]
Mathew CA, Maller S, Maheshwaran. Interactions between magnetic resonance imaging and dental material. J Pharm Bioallied Sci 2013; 5(Suppl 1):S113-S116. [DOI LINK]
Miyata K, Hasegawa M, Abe Y, et al. Radiofrequency heating and magnetically induced displacement of dental magnetic attachments during 3.0 T MRI. Dentomaxillofac Radiol 2012; 41:66-7671. [DOI LINK]
Wilson BJ, O’hare PE, Zacariah J. Implications and considerations of dental materials in MRI: a case report and literature review. Case Reports in Dentistry 2020; Article ID 8891302 [DOI LINK]
Yilmaz S, Aiden MZ. Ex vivo mercury release from dental amalgam after 7.0-T and 1.5-T MRI. Radiology 2018; 288:799-803. [DOI link]
Related Questions
What are susceptibility artifacts?
What are susceptibility artifacts?