Timing of Contrast Bolus
How do you compute the arrival of contrast in a vessel to know when to start the MR acquisition?
|
|
Contrast-enhanced MR angiography (CE-MRA) requires that imaging be initiated at or near the peak time of contrast arrival in the vessel of interest. To estimate the bolus arrival time, (semi)-automated tracking and triggering software are nearly always used. Three basic methods are available: 1) test bolus timing, 2) fluoroscopic triggering, and 3) time-resolved imaging.
With test bolus timing a small (1-2 mL) test dose of contrast is first administered. The vessel is often imaged in cross section even if a different primary plane of imaging is used for the MRA itself. A series of rapidly acquired 2D images is then obtained over the next 20-40 seconds. These images are examined to determine the time course for passage of the test bolus with calculation of optimal time delay and imaging window. The MRA sequence is then run using these parameters with administration of the remainder (~18 mL) of the gadolinium contrast. The bolus timing method can be performed even on older scanners and provides direct evidence the IV and injector are functioning properly. Disadvantages include 1) increased imaging time; 2) wasting of a small amount of contrast during the test injections; and 3) background contamination by gadolinium (can be severe in renal collecting system and bladder).
In fluoroscopic triggering the full bolus of contrast (~20 mL) is administered while a fluoroscopic-like picture of the artery of interest is acquired using a rapid 2D gradient-echo technique. Arrival of the bolus is detected by increased signal in the "fluoroscopic" image. At this time the technologist issues a command to begin the MRA imaging acquisition. The fluoroscopic method offers some advantages in that an experienced technologist can watch the passage of contrast through the heart and proximal vessels to judge to optimal time for imaging to begin.
With test bolus timing a small (1-2 mL) test dose of contrast is first administered. The vessel is often imaged in cross section even if a different primary plane of imaging is used for the MRA itself. A series of rapidly acquired 2D images is then obtained over the next 20-40 seconds. These images are examined to determine the time course for passage of the test bolus with calculation of optimal time delay and imaging window. The MRA sequence is then run using these parameters with administration of the remainder (~18 mL) of the gadolinium contrast. The bolus timing method can be performed even on older scanners and provides direct evidence the IV and injector are functioning properly. Disadvantages include 1) increased imaging time; 2) wasting of a small amount of contrast during the test injections; and 3) background contamination by gadolinium (can be severe in renal collecting system and bladder).
In fluoroscopic triggering the full bolus of contrast (~20 mL) is administered while a fluoroscopic-like picture of the artery of interest is acquired using a rapid 2D gradient-echo technique. Arrival of the bolus is detected by increased signal in the "fluoroscopic" image. At this time the technologist issues a command to begin the MRA imaging acquisition. The fluoroscopic method offers some advantages in that an experienced technologist can watch the passage of contrast through the heart and proximal vessels to judge to optimal time for imaging to begin.
|
Automatic triggering on bolus arrival can also be performed by placing a region-of interest over the vessel to be imaged. Here the scanner, rather than the technologist, identifies the arrival of the contrast bolus when a specified signal threshold (e.g., 20% above baseline) is exceeded. Once the threshold is reached a programmed delay of 3-4 seconds is interposed to allow the peak bolus to arrive before MRA signal acquisition begins.
|
Automatic triggering of contrast bolus using SmartPrep
|
Some form of automatic bolus detection and triggering software, often combined with fluoroscopic visual tracking is offered by every vendor under a different trade name. GE offers both Smart Prep and Fluoro Trigger; Philips offers BolusTrak; Hitachi calls theirs FLUTE ("FLUoro-Triggered Examination); and Canon offers Visual Prep. Siemens uses the term CARE Bolus, which is an acronym carried over from CT angiography standing for "Combined Applications to Reduce (radiation) Exposure".
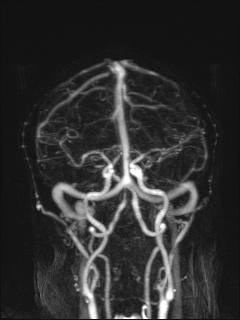
A third method, time-resolved imaging, does not require accurate estimation of the arrival of the contrast bolus. In these techniques, scanning is performed rapidly and repeatedly over the area of interest, with oversampling the central lines of k-space every few seconds. A full dose contrast injection is performed and MR signal acquisition begins a few seconds later. The final set of images constitute a cine display for the evaluation of flow dynamics. The major trade-off for time-resolved methods is between temporal and spatial resolution.

|

|

|

|
|
Series of time-resolved CE-MRA images
Time-resolved CE-MRA techniques include GE's TRICKS and Siemens' TWIST sequences. These methods and their variations will be described in detail in a later Q&A.
References
Foo T, Saranathan M, Prince M, Chenevert TL. Automated detection of bolus arrival and initiation of data acquisition in fast, three-dimensional, gadolinium-enhanced MR angiography. Radiology 1997; 203:275-280. (Description of first automated bolus detection method which became GE's SmartPrep)
Menke J. Carotid MR angiography with traditional bolus timing: clinical observations and Fourier-based modelling of contrast kinetics. Eur Radiol 2009; 19:2654-2662.
Wilman AH, Riederer SJ, King BF, et al. Fluoroscopically triggered contrast-enhanced three-dimensional MR angiography with elliptical centric view order: application to the renal arteries. Radiology.1997;205:137–146.
Foo T, Saranathan M, Prince M, Chenevert TL. Automated detection of bolus arrival and initiation of data acquisition in fast, three-dimensional, gadolinium-enhanced MR angiography. Radiology 1997; 203:275-280. (Description of first automated bolus detection method which became GE's SmartPrep)
Menke J. Carotid MR angiography with traditional bolus timing: clinical observations and Fourier-based modelling of contrast kinetics. Eur Radiol 2009; 19:2654-2662.
Wilman AH, Riederer SJ, King BF, et al. Fluoroscopically triggered contrast-enhanced three-dimensional MR angiography with elliptical centric view order: application to the renal arteries. Radiology.1997;205:137–146.
Related Questions
How is contrast-enhanced MRA performed?
I know there are different view ordering options for MRA, such as linear and elliptical centric. What do these mean, and when is each used?
What is bolus-chasing and how is it used for peripheral MR angiography?
How is contrast-enhanced MRA performed?
I know there are different view ordering options for MRA, such as linear and elliptical centric. What do these mean, and when is each used?
What is bolus-chasing and how is it used for peripheral MR angiography?