Inversion Recovery for myocardial enhancementWhat is the best way to see myocardial enhancement?
|
|
Because of their superior T1 sensitivity, inversion recovery (IR) methods are most frequently used to identify areas of myocardial enhancement. For readers requiring a refresher, the general principles of image formation using IR techniques are more fully explored in another section of the website.
Recovery of cardiac tissues after the 180º-pulse is based is based on their T1 values. An MR signal is generated at the inversion time (TI).
The standard image display method for IR uses magnitude reconstruction. Here the actual direction of Mz (i.e., whether it is points in the +z or −z direction) is irrelevant. The rendered pixel intensity depends only on the magnitude of Mz, not its polarity. Under magnitude reconstruction, air (and any tissue whose magnetization lies is at the zero crossing point at time TI) appears black. This is sometimes illustrated as a "bounce point" diagram, shown right.
|
As a brief review, the IR pulse sequence begins with a 180º-inversion pulse that flips the net magnetization (M) of all tissues into the −z direction. Longitudinal recovery along the +z-axis then occurs, with short T1 tissues recovering faster than long T1 tissues. After a few hundred milliseconds at the inversion time (TI), an MR signal is generated. The strength of this signal for each tissue depends on its longitudinal magnetization (Mz) at time TI.
Magnitude reconstructed IR is often represented on a "bounce point" diagram, showing values of Mz < 0 reflected and displayed as positive.
|
The contrast between tissues in an IR pulse sequence is thus strongly dependent on the TI value chosen. Selecting a TI value where a tissue passes through zero effectively "nulls" that tissue in the image, rendering it dark.
To detect myocardial hyperenhancement (as occurs with infarction and several other diseases) it is desirable to null the signal from nearby normal myocardium. A fixed, predetermined TI value cannot be used, however, as the concentration of gadolinium in both normal myocardium and infarcted tissue decreases over time.
To determine the proper inversion time (TI) to null normal myocardium, an inversion time mapping sequence is frequently performed as illustrated below. This method is based on a principle developed by Look and Locker used in laboratory NMR spectrometers in the 1970's, When applied to modern MRI it is known as TI scout (Siemens) or Cine IR (GE). The technique consists of a centric ordered, segmented series of cine GRE or b-SSFP echoes obtained over 2-3 heart beats, with each segment corresponding to a different TI value. (Details of available methods are described in another Q&A). The series of reconstructed images is visually evaluated to select the best TI for optimal myocardial nulling.
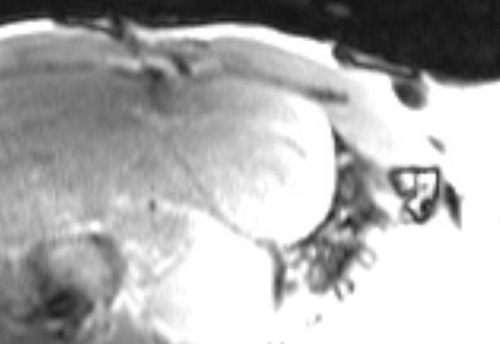
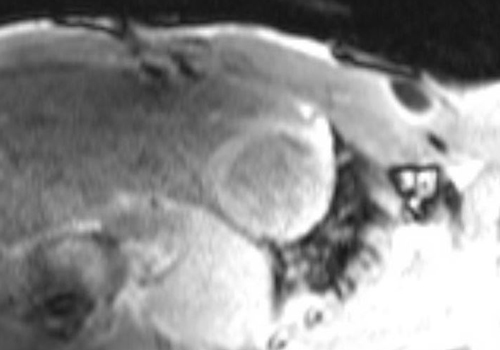
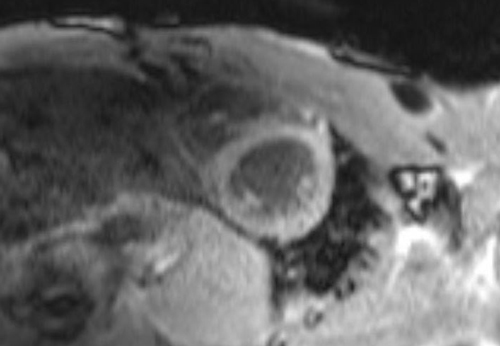
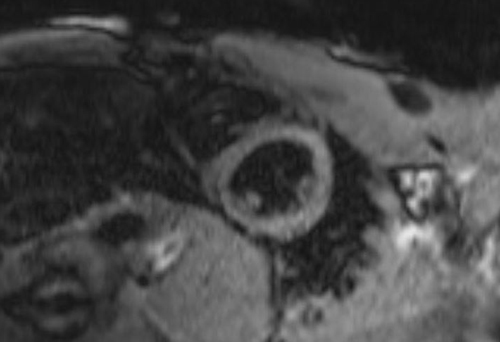
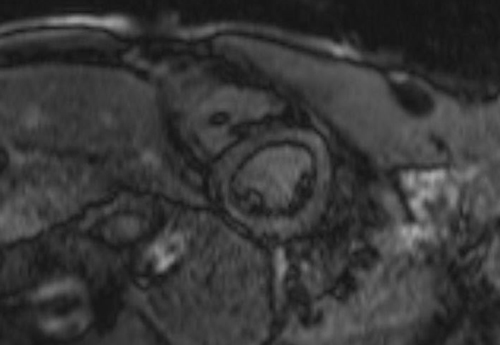
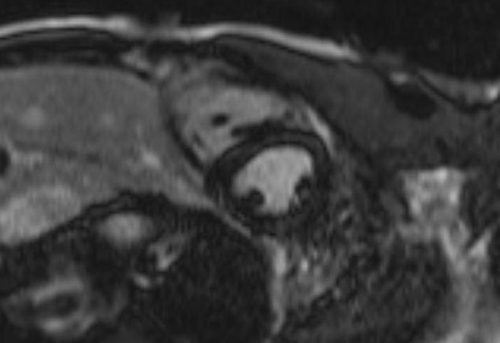

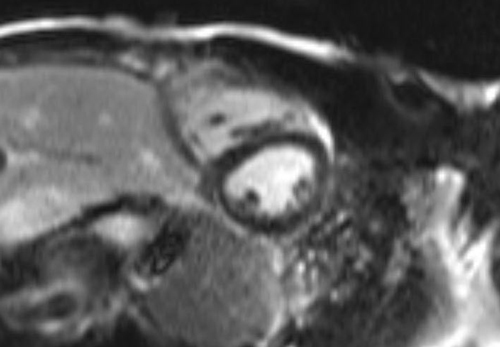
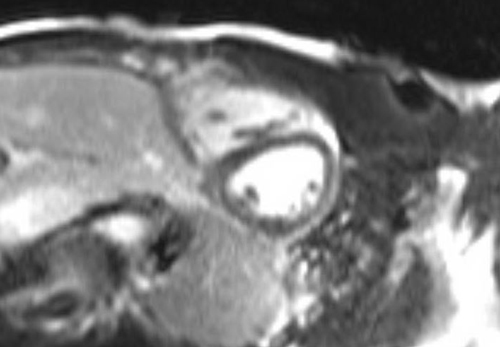
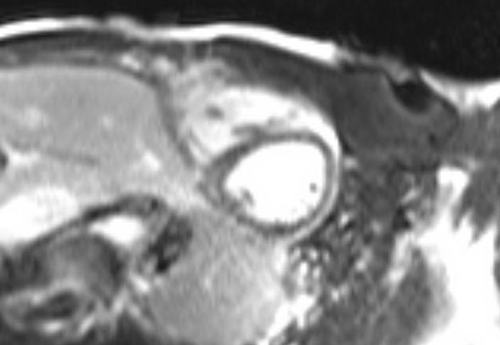
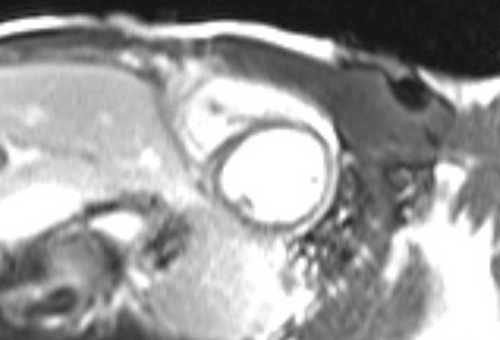
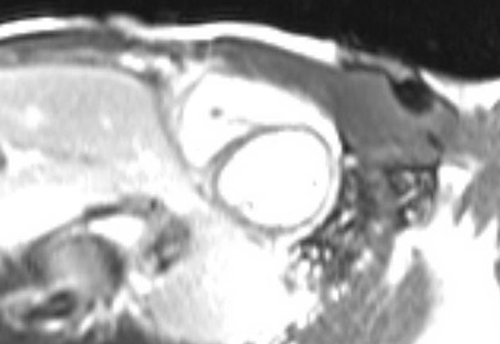
Inversion Time Mapping Sequence ("TI Scout"). Twelve images acquired as part of an inversion time mapping sequence with TI values ranging incrementally from about 200−300 ms. Here the best suppression of normal myocardium can be seen in the second row, third image, corresponding to a TI of 260 ms.
To save time some centers do not perform TI scouting, but prefer to estimate the optimal TI based on experience and dose of contrast related to body weight. Additionally the use of phase-sensitive IR techniques (discussed in the next Q&A) show contrast enhancement over a wide range of values and makes imaging less dependent on an exact value for TI.
References
Coelho-Filho OR, Rickers C, Kwong RY, Jerosch-Herold M. MR myocardial perfusion imaging. Radiology 2013; 266:701-715.
Jerosch-Herold M. Quantification of myocardial perfusion by cardiovascular magnetic resonance. J Cardiovasc Mag Reson 2010; 12:57
Kellman P, Arai AE. Imaging sequences for first past perfusion — a review. J Cardiovasc Mag Reson 2007;9:525-537.
Kim RJ, Shah DJ, Judd RM. How we perform delayed enhancement imaging. J Cardiovasc Magn Reson 2003; 5:505-514.
Shehata ML, Basha TA, Hayeri MR, et al. MR myocardial perfusion imaging: insights on techniques, analysis, interpretation, and findings. Radiographics 2014; 34:1636-1657.
Schwitter J. Myocardial perfusion. J Magn Reson Imaging 2006; 24:953-963.
Coelho-Filho OR, Rickers C, Kwong RY, Jerosch-Herold M. MR myocardial perfusion imaging. Radiology 2013; 266:701-715.
Jerosch-Herold M. Quantification of myocardial perfusion by cardiovascular magnetic resonance. J Cardiovasc Mag Reson 2010; 12:57
Kellman P, Arai AE. Imaging sequences for first past perfusion — a review. J Cardiovasc Mag Reson 2007;9:525-537.
Kim RJ, Shah DJ, Judd RM. How we perform delayed enhancement imaging. J Cardiovasc Magn Reson 2003; 5:505-514.
Shehata ML, Basha TA, Hayeri MR, et al. MR myocardial perfusion imaging: insights on techniques, analysis, interpretation, and findings. Radiographics 2014; 34:1636-1657.
Schwitter J. Myocardial perfusion. J Magn Reson Imaging 2006; 24:953-963.
Vogel-Claussen J, Rochitte CE, Wu KC, et al. Delayed enhancement MR imaging: utility in myocardial assessment. RadioGraphics 2006; 26:796-810.
Related Questions
What is the difference between magnitude and phase-sensitive IR for detecting myocardial enhancement?
How is cardiac T1 mapping performed? When is it useful?
What is the difference between magnitude and phase-sensitive IR for detecting myocardial enhancement?
How is cardiac T1 mapping performed? When is it useful?