Cine Imaging ParametersHow do you choose imaging parameters for a cine cardiac study?
|
|
Modern cine cardiac imaging typically employs a steady-state free precession (SSFP) method consisting of a train of rapidly acquired RF-pulses with echoes formed by balanced imaging gradients. This technique goes under a variety of trade names, including TrueFISP (Siemens), balanced-FFE (Philips), FIESTA (GE), BSARG (Hitachi), and True SSFP (Canon).
|
The use of balanced (symmetric) imaging gradients allows simultaneous refocusing of spin echoes, gradient echoes, and stimulated echoes exactly at the midpoint between RF-pulses. The echo time (TE) is made as short as possible, which on modern systems can be in the 1-2 ms range. RF-flip angle (α) is made large (80°-90°) to accentuate T2/T1 contrast and produce bright blood images.
|
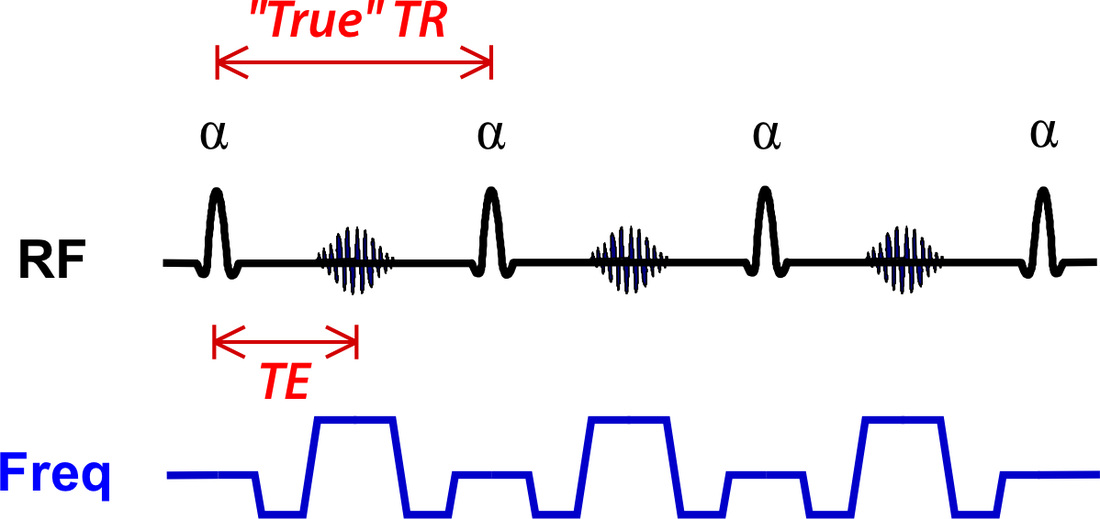
Balanced-SSFP sequence used for cardiac cine
|
In conventional MR imaging, the repetition time (TR) of an SSFP sequence should be defined as the interval between successive RF-pulses. In the diagram above I have labelled this as the "True" TR. In cardiac MRI, however, a different convention is used.
|
The TR value used in cardiac MRI is the time allotted to recording data from an each cardiac frame (segment). If, for example, 7 lines of k-space are acquired for each cardiac frame, the "reported" TR would be 7x the "true" TR. Although called both are called "repetition times", I prefer to think of the "reported" TR used in cardiac MRI as an abbreviation for "temporal resolution."
|
The term repetition time (TR) has a different use in cardiac MRI, better thought of a the time allotted to acquiring data for each frame (segment) rather than "true" TR.
|
Trade-off between temporal resolution and acquisition time. Imaging more cardiac phases mean fewer lines of k-space can be sampled per frame.
|
A trade-off exists between temporal and spatial resolution. The number of cardiac frames (segments) acquired during a single R-R interval and the number of lines per segment are interrelated. As can be seen in the diagram left, if more cardiac phases are desired, fewer lines of k-space can be sampled within each frame, resulting in increased acquisition time.
|
View-sharing creates additional frames by using data from adjacent frames in the cardiac cycle.
|
More cardiac phases can be generated by reusing data from adjacent frames through a process known as view-sharing. As seen in the diagram left, interpolated frames labelled 1.5, 2.5, 3.5, etc. can be created by combining data from neighboring segments.
|
References
Atkinson DJ, Edelman RR. Cineangiography of the heart in a single breath hold with a segmented TurboFLASH sequence. Radiology 1991; 178:357-360. (In the 1990s and early 2000s, cine studies were performed using a spoiled GRE sequence as in the method described here).
Bieri O, Scheffler K. Fundamentals of balanced steady state free precession MRI. J Magn Reson Imaging 2013;38:2-11.
Carr JC, Simonetti O, Bundy J, et al. Cine MR angiography of the heart with segmented true fast imaging with steady-state precession. Radiology 2001; 219:828-834. (First report of a TrueFISP cine sequence, showing its superiority over segmented TurboFLASH methods).
Atkinson DJ, Edelman RR. Cineangiography of the heart in a single breath hold with a segmented TurboFLASH sequence. Radiology 1991; 178:357-360. (In the 1990s and early 2000s, cine studies were performed using a spoiled GRE sequence as in the method described here).
Bieri O, Scheffler K. Fundamentals of balanced steady state free precession MRI. J Magn Reson Imaging 2013;38:2-11.
Carr JC, Simonetti O, Bundy J, et al. Cine MR angiography of the heart with segmented true fast imaging with steady-state precession. Radiology 2001; 219:828-834. (First report of a TrueFISP cine sequence, showing its superiority over segmented TurboFLASH methods).
Related Questions
What is True FISP, and why is it "truer" than regular FISP?
How do they make those movies of the beating heart?
What is True FISP, and why is it "truer" than regular FISP?
How do they make those movies of the beating heart?