MR Safety: Skeletal Traction and Halo VestsWhat are the MR safety issues for patients with skeletal or cervical traction?
|
|
|
Skeletal traction is principally used for reducing deformity and stabilizing complex fractures or dislocations, often as a temporizing measure prior to open reduction and surgical internal fixation. A typical apparatus, shown right, illustrates the use of traction to to treat a femur fracture. A thin metal rod (e.g., Steinmann pin, Kirschner "K"-wire) is first percutaneously screwed through the upper tibia, then connected with a bow to a cable and pulley system to which weights are attached.
|
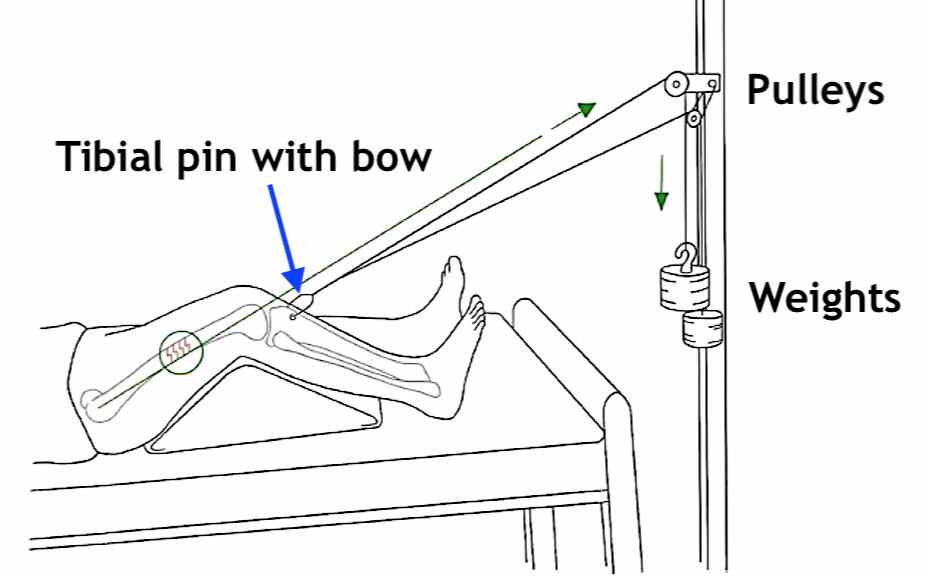
Traction apparatus for a femur fracture
(Modified from Choudhry under CC BY) |
Although completely MRI-compatible skeletal traction systems are available, most facilities have legacy components including cast-iron weights and stainless steel bows that are MR Unsafe. Caution should even be directed concerning "sandbag"-type weights, that occasionally contain iron pellets instead of sand or lead. Evaluation of the entire traction system with a hand-held magnet prior to entry into the MRI scanner room is advised.
Cervical Spine Traction and Halo Vests
|
Unstable upper cervical spine fractures and dislocations are often initially treated with mechanical traction. Traction pins are inserted into the outer table of the skull by means of Gardner-Wells-type tongs (2 pins) or, more commonly, by an oval 4-pin halo device. Once satisfactory alignment has been obtained, the halo can be converted into a halo vest (which may be the definitive treatment for certain fractures in lieu of surgery).
General MR safety issues similar to those discussed for other external fixation devices (see related Q&A) apply to halo vests, including magnetic displacement/torque and eddy-current induced vibrations. Many models are MR Unsafe.
|

MR Conditional Halo Vest
|
An additional safety concern is the possibility of scalp burns at the site of halo pins from induced currents. As such MR conditional halos and halo vests must have rings and supports that are not only made out of non-ferrous materials, but also non-conductive ones, such as fiberglass or carbon fiber composites. To further prevent burns, the scalp pins of at least one halo manufacturer (Össur) are ceramic-tipped.
References
Choudhry B, Leung B, Filips E, Dhaliwal K. Keeping the traction on in orthopaedics. Cureus 2020; 12:e10034 [DOI LINK]
Graf H, Lauer UA, Schick F. Eddy-current induction in extended metallic parts as a source of considerable torsional moment. J Magn Reson Imaging 2006; 23:585-590. [DOI LINK]
Hartwell RC, Shellock FG. MRI of cervical fixation devices: sensation of heating caused by vibration of metallic components (letter). J Magn Reson Imaging 1997; 7:771-2. [DOI LINK]
Jones AAM, Arena MJ, Zoller JH III, et al. Potential hazard: traction weights and magnetic resonance imaging. Spine 1991; 16:364-5.
Kim LJ, Sonntag VK, et al. Scalp burns from halo pins following magnetic resonance imaging. Case report. J Neurosurg 2003; 99:186.
Liu Y, Shen J, Kainz W, et al. Numerical investigations of MRI RF field induced heating for external fixation devices. BioMedical Engineering OnLine 2013; 12:12. [DIRECT LINK]
Luechinger R, Boesiger P, Disegi JA. Safety evaluation of large external fixation clamps and frames in a magnetic resonance environment. J Biomed Mater Res Part B: Appl Biomater 2007; 82B:17–22. [DOI LINK]
Mani RL. Potential hazard of metal-filled sandbags in MR imaging (letter). Radiology 1992; 182:286-287.
Mansour A, Block J, Obremskey W: A cadaveric simulation of distal femoral traction shows safety in magnetic resonance imaging. J Orthop Trauma 2009;23: 658-662.
Milby JN, Bible JE, Mosher TJ, Garner MR. External orthopedic implants in the magnetic resonance environment: current concepts and controversies. J Am Acad Orthopedic Surg 2020; 28:e139-e144. [DOI LINK]
Perry KJ, Massey PA, Simoncini A, Barton RS. MRI safety of external fixation devices: a review of the literature. Curr Orthop Pract 2018; 29:302-307.
Choudhry B, Leung B, Filips E, Dhaliwal K. Keeping the traction on in orthopaedics. Cureus 2020; 12:e10034 [DOI LINK]
Graf H, Lauer UA, Schick F. Eddy-current induction in extended metallic parts as a source of considerable torsional moment. J Magn Reson Imaging 2006; 23:585-590. [DOI LINK]
Hartwell RC, Shellock FG. MRI of cervical fixation devices: sensation of heating caused by vibration of metallic components (letter). J Magn Reson Imaging 1997; 7:771-2. [DOI LINK]
Jones AAM, Arena MJ, Zoller JH III, et al. Potential hazard: traction weights and magnetic resonance imaging. Spine 1991; 16:364-5.
Kim LJ, Sonntag VK, et al. Scalp burns from halo pins following magnetic resonance imaging. Case report. J Neurosurg 2003; 99:186.
Liu Y, Shen J, Kainz W, et al. Numerical investigations of MRI RF field induced heating for external fixation devices. BioMedical Engineering OnLine 2013; 12:12. [DIRECT LINK]
Luechinger R, Boesiger P, Disegi JA. Safety evaluation of large external fixation clamps and frames in a magnetic resonance environment. J Biomed Mater Res Part B: Appl Biomater 2007; 82B:17–22. [DOI LINK]
Mani RL. Potential hazard of metal-filled sandbags in MR imaging (letter). Radiology 1992; 182:286-287.
Mansour A, Block J, Obremskey W: A cadaveric simulation of distal femoral traction shows safety in magnetic resonance imaging. J Orthop Trauma 2009;23: 658-662.
Milby JN, Bible JE, Mosher TJ, Garner MR. External orthopedic implants in the magnetic resonance environment: current concepts and controversies. J Am Acad Orthopedic Surg 2020; 28:e139-e144. [DOI LINK]
Perry KJ, Massey PA, Simoncini A, Barton RS. MRI safety of external fixation devices: a review of the literature. Curr Orthop Pract 2018; 29:302-307.
Related Questions
Can one safely scan patients with total joints and other orthopedic hardware like plates and screws ?
How can you tell if an external fixation device is safe for MRI?
Can one safely scan patients with total joints and other orthopedic hardware like plates and screws ?
How can you tell if an external fixation device is safe for MRI?