T2-Imaging/Mapping
How are T2-weighted imaging and mapping used for cardiac diagnosis?
|
|
A large portion of cardiology practice involves the diagnosis and treatment of acute coronary syndrome (ACS). Acute myocardial infarction produces myocardial edema, manifest by increased free water content with significantly prolonged T2 values. T2-weighted MR imaging has been shown to help differentiate ACS from remote infarction and non-ACS causes of chest pain. Although controversy exists, many consider T2-hyperintense regions to delineate an "area at risk" for ischemic myocardial injury. In conjunction with late gadolinium enhancement, T2-based images may be used to quantify myocardial salvage and the success of coronary revascularization surgery.
Prolonged T2, however, is not specific for acute myocardial infarction. It can be seen in chronic infarction as well as acute myocarditis, cardiomyopathies, myocardial contusion, transplant rejection, sarcoidosis, and various infiltrative diseases.
Conversely, short T2 areas (dark on T2-weighted images) may indicate myocardial hemorrhage and areas of microvascular obstruction within an infarct. These features have been associated with poor LV remodeling and worse clinical outcomes.
Several pulse sequences are available for T2-weighted imaging. The oldest are fast (turbo) spin-echo sequences with long TR's/ TE's. These are typically preceded by an inversion module to suppress blood (double inversion recovery, DIR) and/or fat (triple inversion recovery, TIR). The latter method has contrast features similar to short-TI inversion recovery (STIR) imaging in that T1- and T2- signal contributions are additive.
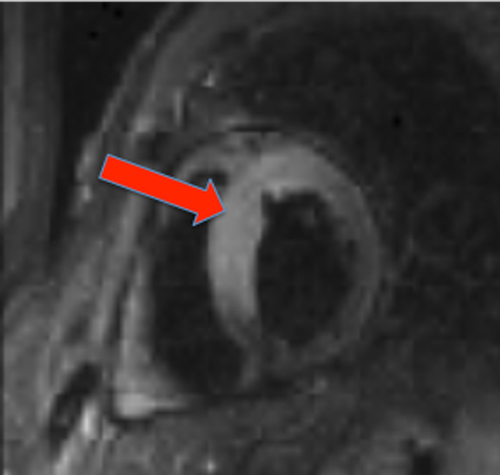
Septal edema on STIR in patient with recent
acut e myocardial infarction |
Although dozens of T2 mapping sequences have been developed at research sites, the most widely used worldwide are those which are commercially available. These are all 2D include: single-shot T2-prepared bSSFP or T2p-GRE, multi-echo fast spin echo (multi-echo FSE), and gradient spin echo (GraSE). The first two have been recommended by the Society for Cardiovascular Magnetic Resonance.
|
Assessment of T2 hyperintensities are by nature subjective, and MR artifacts may both mimic or obscure true abnormalities. Such artifacts include: 1) surface coil nonuniformities creating variable T2 signal across the myocardium; 2) bright subendocardial rims on DIR/TIR due to stagnant blood; and 3) loss of signal from the posterior wall due to cardiac movement.
To overcome some of these difficulties and allow more consistency of diagnosis, T2-mapping has been recommended. T2-mapping is typically performed using a balanced SSFP readout sequence preceded by a multinomial T2-preparation module. Signals are sampled at several different TE's and fitted to an exponential decay curve of the form:
Si = Mo e−TEi / T2
to determine T2. The results are displayed on a pixel-by-pixel base in a color map, from which T2-values can be directly measured.
At 1.5T the T2 of the normal heart is approximately 45-55 ms. Exact threshold values for edema detection have not been firmly established, but those ≥ 70 ms are generally considered abnormal.
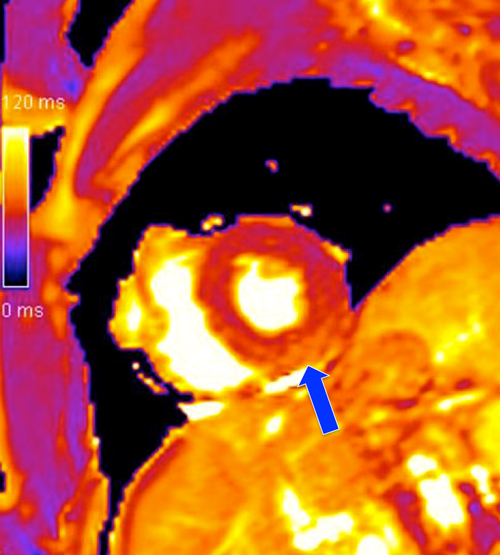
T2-map shows inferior wall ischemia manifest by prolonged T2 values (>100 ms)
|
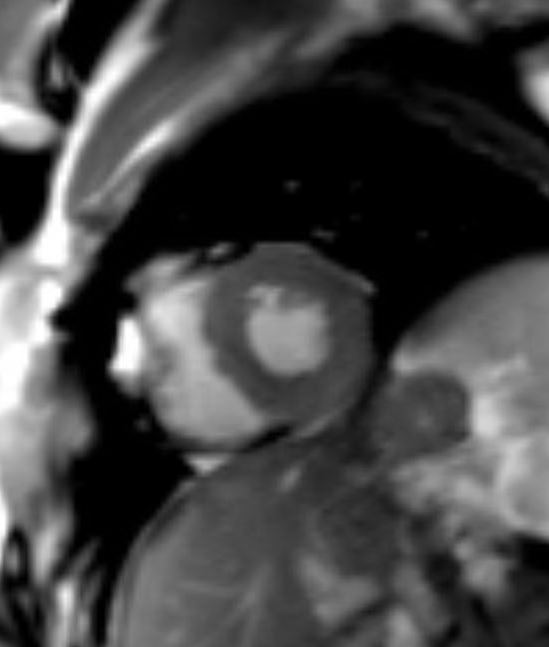
T2-prepared SSFP image does not demonstrate myocardial high signal
|
References
Aletras AH, Kellman P, Derbyshire JA, Arai AE. ACUT2E TSE-SSFP: a hybrid method for T2-weighted imaging of edema in the heart. Magn Reson Med 2008; 59:229-235.
Croisille P, Kim HW, Kim RJ. Controversies in cardiovascular MR imaging. T2-weighted imaging should not be used to delineate the area at risk in ischemic myocardial injury. Radiology 2012; 265:12-22.
Eitel I, Friedrich MG. T2-weighted cardiovascular magnetic resonance in acute cardiac disease. J Cardiovasc Magn Reson 2011; 13:13.
Giri S, Chung Y-C, Merchant A, et al. T2 quantification for improved detection fo myocardial edema. J Cardiovasc Magn Reson 2009; 11:56.
McAlindon EJ, Pufulete M, Harris JM, et al. Measurement of myocardium at risk with cardiovascular MR: comparison of techniques for edema imaging. Radiology 2015; 275:61-70. (In setting of STEMI, myocardial edema is detected most reproducibly using T2 mapping over STIR and early gadolinium enhancement).
Messroghli DR, Moon JC, Ferreira VM, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: a consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson. 2017;19:75.
O’Brien AT, Gil KE, Varghese J, et al. T2 mapping in myocardial disease: a comprehensive review. J Cardiovasc Magn Reson 2022;24:33 [DOI LINK]
Verhaert D, Thavendiranathan P, Giri S, et al. Direct T2 quantification of myocardial edema in acute ischemic injury. JACC Cardiovasc Imaging 2011; 4:269-278.
Aletras AH, Kellman P, Derbyshire JA, Arai AE. ACUT2E TSE-SSFP: a hybrid method for T2-weighted imaging of edema in the heart. Magn Reson Med 2008; 59:229-235.
Croisille P, Kim HW, Kim RJ. Controversies in cardiovascular MR imaging. T2-weighted imaging should not be used to delineate the area at risk in ischemic myocardial injury. Radiology 2012; 265:12-22.
Eitel I, Friedrich MG. T2-weighted cardiovascular magnetic resonance in acute cardiac disease. J Cardiovasc Magn Reson 2011; 13:13.
Giri S, Chung Y-C, Merchant A, et al. T2 quantification for improved detection fo myocardial edema. J Cardiovasc Magn Reson 2009; 11:56.
McAlindon EJ, Pufulete M, Harris JM, et al. Measurement of myocardium at risk with cardiovascular MR: comparison of techniques for edema imaging. Radiology 2015; 275:61-70. (In setting of STEMI, myocardial edema is detected most reproducibly using T2 mapping over STIR and early gadolinium enhancement).
Messroghli DR, Moon JC, Ferreira VM, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: a consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson. 2017;19:75.
O’Brien AT, Gil KE, Varghese J, et al. T2 mapping in myocardial disease: a comprehensive review. J Cardiovasc Magn Reson 2022;24:33 [DOI LINK]
Verhaert D, Thavendiranathan P, Giri S, et al. Direct T2 quantification of myocardial edema in acute ischemic injury. JACC Cardiovasc Imaging 2011; 4:269-278.
Related Questions
How is cardiac T1 mapping performed? When is it useful?
How and why is T2*-myocardial mapping performed?
How is cardiac T1 mapping performed? When is it useful?
How and why is T2*-myocardial mapping performed?