Why/How Stress Test
Why would you want to do a stress MRI? How is it performed?
|
|
Stress perfusion MRI is typically performed in patients with known or suspected coronary atherosclerosis to identify areas of inducible ischemia, to predict cardiac prognosis, to stratify risk for non-cardiac surgery, or to assess myocardial viability. The underlying principle is that myocardial dysfunction (impaired wall motion and/or perfusion) may sometimes be seen only when the distal myocardial capillary bed is maximally dilated during cardiac stress.
In echocardiography suites stress is typically induced by exercise using a treadmill or stationary bicycle. As these devices are impractical in the MR imaging suite, modern CMR employs pharmacologic "stress" created by intravenous infusion of a vasodilator (adenosine/regadenoson) or positive inotrope (dobutamine).
|
Gadolinium contrast to assess perfusion is administered to all patients except those with severe allergies or renal insufficiency. Delayed T1-weighted images at 10-20 minutes are also usually acquired to look for delayed myocardial enhancement. Both stress and rest MR images are carefully compared, with disparities between wall motion, perfusion, and delayed enhancement essential for diagnosis.
|
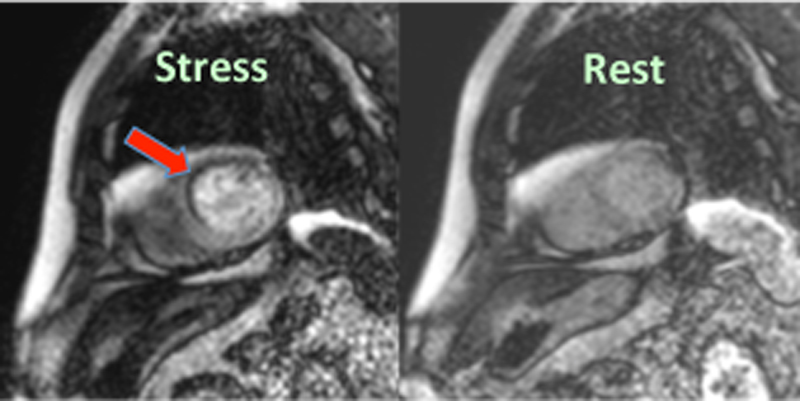
Inducible ischemia (dark area, arrow) in the anteroseptal cardiac wall noted on perfusion study during stress but not at rest.
|
Prior to performing a stress perfusion procedure, the following preparatory steps are essential
- Renal function testing. Because of the risk of nephrogenic systemic fibrosis, gadolinium cannot be given safely to patients with severe renal disease and should be administered in reduced dosage for patients with renal insufficiency. If there is any suspicion of renal disease a recent estimated glomerular filtration rate (eGFR) should generally be obtained prior to gadolinium administration.
- Cardiac troponin testing. Cardiac troponins are enzymes released by damaged myocardium. As pharmacological stress testing is generally contraindicated after a recent myocardial infarction, measurement of serum troponins should be performed in the appropriate clinical setting.
- Medical history review. In addition to recent myocardial infarction, pharmacological stress testing may be contraindicated in patients with acute myocarditis/pericarditis, progressive unstable angina, rapid arrhythmias, 2nd or 3rd degree AV block, and other disorders. Questioning the patient about reactive airway disease should always be performed, as regadenoson (Lexiscan) would likely be preferred over adenosine in this clinical scenario.
- Informed consent. Pharmacological stress testing confers additional rare but significant risks to the patient, including myocardial infarction, arrhythmias, seizures, stroke, and even death. Hence a formal signed consent and discussion with the patient is required.
- Start 2 IVs. Gadolinium and adenosine cannot be given through the same line, so two separate IVs are required. Separate lines are optional if regadenoson or dobutamine is used.
- Avoidance of stimulants. Patients should be advised not to consume stimulants such as coffee, tea, caffeinated sodas, energy drinks, and chocolate within 12-24 hours of the scan. Dipyridamole (Persantine) and dipyridamole-containing medications (Aggrenox) should generally be discontinued for 48 hours. All these stimulants and medications can interfere with the efficacy of the pharmacological stress testing and interpretation of the examination.
- Equipment, staffing, and safety. Stress CMR carries small but significant risks and so a team of nurses, techs, and cardiologists must be ready to mange acute complications such as hypotension, myocardial ischemia, arrhythmias, and respiratory insufficiency. MRI-compatible monitoring equipment, drugs (especially β-blockers, bronchodilators, aminophylline, and nitroglycerine), defibrillator, and full emergency cart with temporary pacemaker should be readily available. An emergency resuscitation policy should be in place with training/practice sessions for staff to handle situations requiring urgent response.
The usual stress-rest CMR protocol varies somewhat among centers and by specific clinical indication, but generally follows a sequence of steps similar to those listed below:
- Anatomic survey using SSFP localizers plus 2-, 3-, and 4-chamber dark/bright blood views.
- Resting wall motion study using SSFP-cine (short axis view essential plus others)
- Stressor agent infusion. Timing and dose varies with drug: adenosine (140 μg/ml/min) continuous IV over 4 minutes or regadenoson 0.4 mg IV push.
- First "half dose" gadolinium injection. We prefer gadobenate (MultiHance®) at 0.05 mmol/kg due to its high relaxivity and safety profile. This is one-half of the "standard" (0.1 mmol/kg) dose, the other half given later in the procedure.
- Stress perfusion module acquiring ~50 images using first-pass SSFP or GRE technique.
- Optional stress wall motion study (identical to step 2)
- Wait 10 minutes. May perform other anatomic or flow imaging during this period.
- Second "half-dose" gadolinium injection.
- Resting perfusion module. Identical to step 5 but without adenosine/stressor agent.
- Wait 10 minutes (to allow Gd uptake into myocardium)
- Delayed enhancement imaging. TI-scout to determine optimal TI for myocardial suppression, followed by magnitude and phase-corrected IR imaging with optional T1-mapping.
References
Hundley WG, Morgan TM, Neagle CM, et al. Magnetic resonance imaging determination of cardiac prognosis. Circulation 2002; 106:2328-2333. (presence of inducible ischemia with dobutamine/atropine can be used to forecast myocardial infarction or cardiac death).
Kramer CM, Barkhausen J, Flamm SD, et al. Standardized cardiovascular magnetic resonance (CMR) protocols 2013 update. J Cardiovasc Magn Reson 2013: 15:91.
von Knobelsdorff-Brenkenhoff F, Schulz-Menger J. Cardiovascular magnetic resonance imaging in ischemic heart disease. J Magn Reson Imaging 2012; 36:20-38.
Hundley WG, Morgan TM, Neagle CM, et al. Magnetic resonance imaging determination of cardiac prognosis. Circulation 2002; 106:2328-2333. (presence of inducible ischemia with dobutamine/atropine can be used to forecast myocardial infarction or cardiac death).
Kramer CM, Barkhausen J, Flamm SD, et al. Standardized cardiovascular magnetic resonance (CMR) protocols 2013 update. J Cardiovasc Magn Reson 2013: 15:91.
von Knobelsdorff-Brenkenhoff F, Schulz-Menger J. Cardiovascular magnetic resonance imaging in ischemic heart disease. J Magn Reson Imaging 2012; 36:20-38.
Related Questions
Are there any special measures needed in preparing a patient for a cardiac MRI exam?
How does a myocardial perfusion study MRI work? Why would you want to do one?
Our cardiac MRI binder contains over a dozen different protocols. Can you make sense of these?
Several drugs are available to perform cardiac stress. Which one should I use?
Are there any special measures needed in preparing a patient for a cardiac MRI exam?
How does a myocardial perfusion study MRI work? Why would you want to do one?
Our cardiac MRI binder contains over a dozen different protocols. Can you make sense of these?
Several drugs are available to perform cardiac stress. Which one should I use?