Semi-Quantitative Parameters
What parameters can be extracted from the DSC intensity curve?
|
|
A number of semi-quantitative perfusion parameters can be obtained by analysis of DSC signal intensity curves for each voxel during passage of the contrast bolus. These parameters are easy to calculate and hence are widely used. However, they lack precision and consistency, being highly dependent on the efficiency/compactness of the contrast bolus. The absolute values of these parameters have little meaning by themselves, but can be helpful in a relative sense (such as comparing corresponding regions on two sides of the brain). The most common of these so-called "summary" parameters are illustrated and defined below.
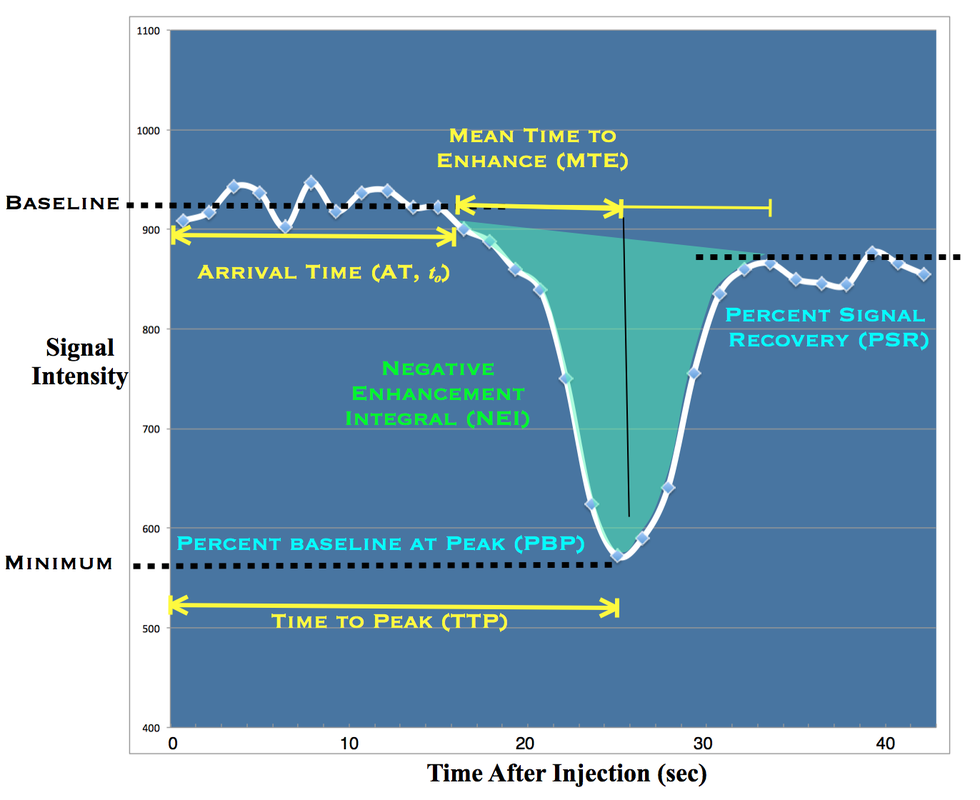
Simplified semiquantitative analysis of DSC signal intensity curves
- Arrival Time (AT, to) is the interval between intravenous contrast injection and its first detection in tissue (or in a large feeding artery). Because MR signals vary randomly due to noise and motion, a dozen or more time points must be averaged prior to contrast arrival to establish a baseline. An arbitrary detection threshold is then set (e.g., 5% below baseline) to define contrast arrival. Alternatively, this threshold may be set manually by visual inspection of the signal intensity curve. However calculated, AT reflects the sum of all processes leading to tissue delivery of contrast (injection rate, cardiac output, region blood flow, etc). Significantly different arrival times of contrast to the two sides of the brain, for example, might reflect unilateral carotid artery stenosis.
- Time to Peak (TTP) is typically defined as the time from initial contrast injection to peak (maximal) signal loss within the organ of interest. TTP has the same uses and limitations as AT but is superior because the peak is easily identified without need to set an arbitrary detection threshold for first arrival. In some software applications, TTP does not include the arrival time, being defined as the interval between first detection of contrast (to) and peak signal loss.
- Negative Enhancement Integral (NEI) is the total area ("integral") under the signal intensity curve during first pass of gadolinium, sometime known by its synonym, Area Under Curve (AUC). NEI reflects the total amount of contrast transiting through the regional vascular system and is roughly proportional to blood volume. Because of recirculation effects explained in the prior Q&A, the baseline does not return to normal at the end of the first pass. An arbitrary decision must then be to made as to define the right hand limit of integration as well as how to handle the shifting baseline. Often mathematical models of the signal intensity curve (such as the gamma variate function) are used to correct for recirculation and baseline shift effects and make NEI calculations more consistent.
- Mean Time to Enhance (MTE) represents the average time for the entire bolus of injected contrast to pass through a region of tissue. Absolute values of MTE are therefore highly dependent on the shape (compactness) of the arriving contrast bolus and to a lesser degree on tissue perfusion. Although frequently confused, it is important to recognize that MTE is not the same as Mean Transit Time (MTT), which reflects the average time for a single contrast molecule (not the entire bolus) to pass through tissue. In simulations, MTE can be up to 3x longer than true MTT. The uncertainty is compounded in that vendors have slightly different names and methods for computing MTE, including calculating the first moment (centroid) of the NEI or using its full width at half maximum (FWHM). Some software applications also provide a simplified estimate of relative blood flow (rBF) from this data, calculated as NEI/MTE. Although an analog for true blood flow (BF = BV/MTT), the limitations and errors in this approach are readily apparent.
- Percent Baseline at Peak (PBP) and Percent Signal Recovery (PSR) are defined respectively as the ratios of signal intensity at minimum (peak) or during the recirculation phase (recovery) divided by their initial (baseline) values. Easy to calculate but these parameters reflect a mixture of experimental and physiological phenomena, so are infrequently used.
Time-to-peak (TTP, left) and negative enhancement integral (NEI, right) maps generated on a pixel-by-pixel basis directly from first-pass signal intensity curves in a DSC study. Although their absolute values are meaningless, they are easy to calculate and may be useful in a relative sense to compare perfusion in corresponding brain regions.
|
To derive more quantifiable maps such as blood flow and blood volume more sophisticated mathematical processing is required. This is the subject of several additional Q&A's that follow.
References
Jahng G-H, Li K-L, Ostergaard l, Calamante F. Perfusion magnetic resonance imaging: a comprehensive update on principles and techniques. Korean J Radiol 2014; 15:554-577.
McGehee BE, Pollock JM, Maldjian JA. Brain perfusion imaging: how does it work and what should I use? J Magn Reson Imaging 2012; 36:1257-1272.
Perthen JE, Calamante F, Gadian DG, Connelly A. Is quantification of bolus tracking MRI reliable without deconvolution? Magn Reson Med 2002; 47:62-67. (The answer is NO).
Welker K, Boxerman J, Kalnin A, et al. ASFNR recommendations for clinical performance of MR dynamic susceptibility contrast perfusion imaging of the brain. AJNR Am J Neuroradiol 2015; 36: E41-E51.
Jahng G-H, Li K-L, Ostergaard l, Calamante F. Perfusion magnetic resonance imaging: a comprehensive update on principles and techniques. Korean J Radiol 2014; 15:554-577.
McGehee BE, Pollock JM, Maldjian JA. Brain perfusion imaging: how does it work and what should I use? J Magn Reson Imaging 2012; 36:1257-1272.
Perthen JE, Calamante F, Gadian DG, Connelly A. Is quantification of bolus tracking MRI reliable without deconvolution? Magn Reson Med 2002; 47:62-67. (The answer is NO).
Welker K, Boxerman J, Kalnin A, et al. ASFNR recommendations for clinical performance of MR dynamic susceptibility contrast perfusion imaging of the brain. AJNR Am J Neuroradiol 2015; 36: E41-E51.