Black Blood Double IR
When is double inversion recovery used for cardiac imaging? How does it work?
|
|
Double inversion recovery (DIR) is a type of "black blood" technique useful for visualizing the walls of the cardiac chambers and blood vessels (including the coronary arteries).
As the name implies, the sequence involves application of two RF-inversion pulses in close succession after an EKG trigger. The first inverting pulse is spatially non-selective, while the second pulse is spatially selective.
Dark blood double IR sequence. After the two inversion pulses, tissue within a slice is unaffected, but the magnetization of blood outside the slice is inverted. As this blood flows into the slice for imaging, it produces no signal since TI is chosen to be null its signal. The image acquisition module is typically 2D fast (turbo) spin echo.
The term nonselective means that the first 180°-pulse inverts all spins within the entire active volume of the transmit coil. The second 180°-pulse is spatially selective, meaning that its effects are restricted to the single slice being imaged. The second RF-pulse thus restores longitudinal magnetization for both blood and myocardium within the imaging slice. For spins outside the slice, however, the longitudinal magnetization remains inverted.
Over the next several hundred msec, two events occur simultaneously: 1) inverted blood initially outside the imaged slice undergoes T1-recovery of its longitudinal magnetization, passing through zero as it attempts to realign with Bo; and 2) this outside blood flows into and replaces blood within the imaged slice.
The inversion time (TI) is chosen so that the magnetization of this inflowing blood passes through zero at the start of image acquisition. For cardiac imaging at 1.5T with a heart rate of 60 BPM, this typically means a TInull of approximately 650 msec. If the HR is too fast, TI must be reduced. Some systems do this automatically using a software-based blood suppression TI calculation.
The most commonly used imaging sequence in conjunction with this double IR method is fast (turbo) spin echo with a relatively short TEeff (≈ 40 msec). Alternatively, a segmented k-space gradient echo or echo-planar sequence may also be used.
Over the next several hundred msec, two events occur simultaneously: 1) inverted blood initially outside the imaged slice undergoes T1-recovery of its longitudinal magnetization, passing through zero as it attempts to realign with Bo; and 2) this outside blood flows into and replaces blood within the imaged slice.
The inversion time (TI) is chosen so that the magnetization of this inflowing blood passes through zero at the start of image acquisition. For cardiac imaging at 1.5T with a heart rate of 60 BPM, this typically means a TInull of approximately 650 msec. If the HR is too fast, TI must be reduced. Some systems do this automatically using a software-based blood suppression TI calculation.
The most commonly used imaging sequence in conjunction with this double IR method is fast (turbo) spin echo with a relatively short TEeff (≈ 40 msec). Alternatively, a segmented k-space gradient echo or echo-planar sequence may also be used.
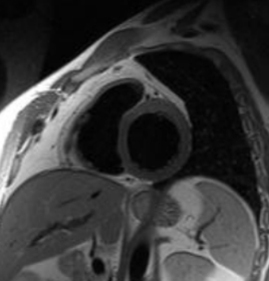
Short-axis double IR image of heart
|
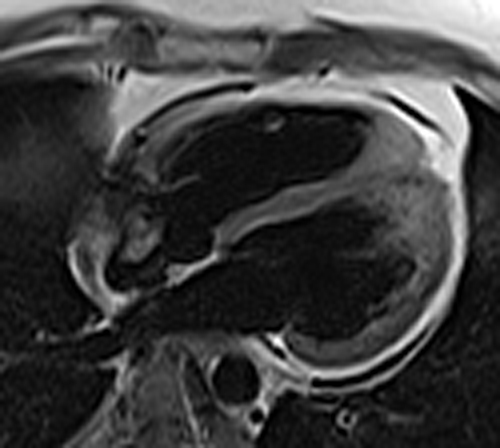
Long-axis double IR image of heart
|
Limitations of the DIR technique include prolonged imaging times and sequence-specific artifacts.
First relatively long inversion times are necessary especially at slower heart rates to achieve sufficient nulling of blood. These long TI values may conflict with optimal trigger delay, forcing adoption of a suboptimal imaging protocol. With long TI's a repetition time (TR) of two heart beats may be required for effective blood suppression. The end result is that imaging of a single coronary artery might take in excess of 10 minutes to image using the DIR method.
First relatively long inversion times are necessary especially at slower heart rates to achieve sufficient nulling of blood. These long TI values may conflict with optimal trigger delay, forcing adoption of a suboptimal imaging protocol. With long TI's a repetition time (TR) of two heart beats may be required for effective blood suppression. The end result is that imaging of a single coronary artery might take in excess of 10 minutes to image using the DIR method.
|
Blood suppression may also be compromised if the plane of imaging is not perpendicular to the direction of flow. This is illustrated the image (right) where signal in the cardiac chambers is well-suppressed but that in the descending aorta (red arrow) is not. Here flow in the aorta lies within the plane of imaging, and aortic blood is is not completely replenished between the two inversion pulses. A similar phenomenon may occur in tortuous or slowly-flowing arteries. Sometimes an artifactual high-intensity band may appear along the periphery of an artery due to slow laminar flow at the boundary between the vessel wall and its lumen.
|

Incomplete blood suppression of in-plane flow in thoracic aorta on this DIR study.
|
References
Edelman RR, Chien D, Kim D. Fast selective black blood MR imaging. Radiology 1991; 181:655-660.
Liu Y, Riederer SJ, Ehman RL. Magnetization-prepared cardiac imaging using gradient echo acquisition. Magn Reson Med 1993; 30:271-275.
Siemens. Cardiac MRI Morphology 2004. (Slide-based review of dark blood technique with optimization suggestions and imaging examples).
Edelman RR, Chien D, Kim D. Fast selective black blood MR imaging. Radiology 1991; 181:655-660.
Liu Y, Riederer SJ, Ehman RL. Magnetization-prepared cardiac imaging using gradient echo acquisition. Magn Reson Med 1993; 30:271-275.
Siemens. Cardiac MRI Morphology 2004. (Slide-based review of dark blood technique with optimization suggestions and imaging examples).
Related Questions
Why go to the trouble of using a double IR method to suppress blood? Couldn't blood be suppressed with a single carefully selected TI value?
Isn't double inversion recovery enough? Why would you want to do triple IR?
Why go to the trouble of using a double IR method to suppress blood? Couldn't blood be suppressed with a single carefully selected TI value?
Isn't double inversion recovery enough? Why would you want to do triple IR?