ASL Imaging ParametersHow should imaging parameters be chosen to optimize an ASL acquisition?
|
|
|
The choice of optimal imaging parameters is dependent upon the exact ASL method utilized (2D vs 3D, PICORE vs FAIR vs pCASL, etc.) Even small variations of each sequence (such as type of background suppression and pulse shaping) will affect parameter selection. Expected blood flows should also be considered, in that children have more robust circulations than adults. Many choices are empirical, so one should always begin with parameters recommended by the vendor or pulse sequence designer. That said, a few general rules are applicable to each implementation.
|
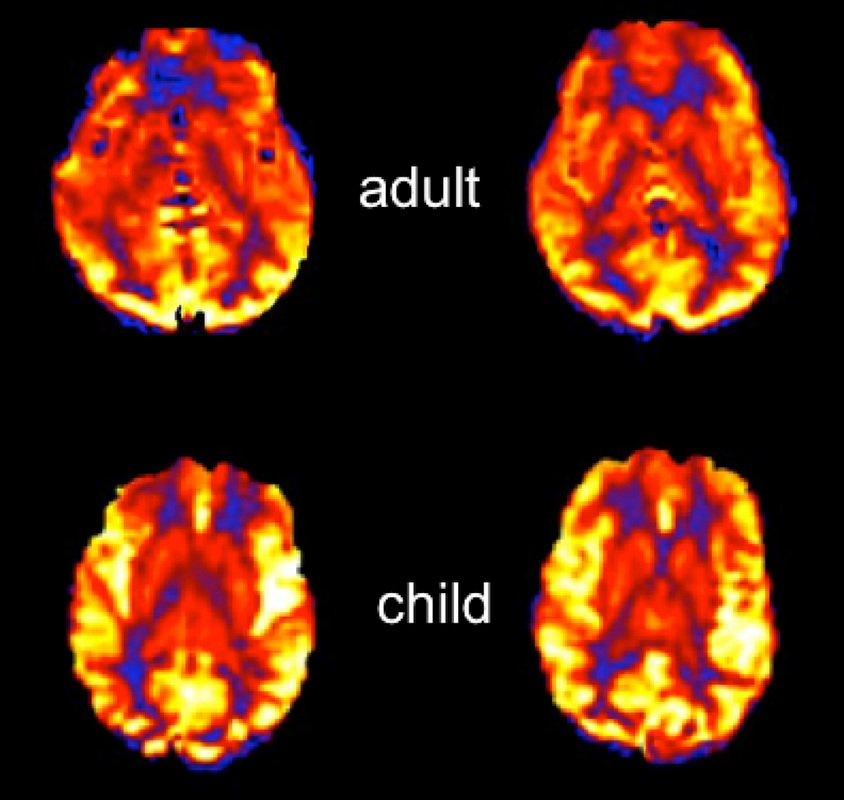
Children have higher relative blood flows and shorter mean transit times than adults
|
- Plane of imaging. All ASL methods perform best when imaging is acquired in transverse planes perpendicular to the imaging slab.
- Equipment. Use highest field strength available. ASL techniques are signal-to-noise ratio (SNR) limited, so all perform better at 3.0T than at 1.5T or below. Multi-channel coils are mandatory. A low-level of parallel acceleration (R≈2) may be useful for 3D acquisitions, but should be used judiciously in 2D methods due to its SNR penalty.
- Repetition time (TR) should be long enough to allow substantial relaxation of labeled spins between acquisitions, typically greater than 3500 ms.
- Minimum echo time (TE) should always be used to preserve signal from T2/T2* decay.
- Spatial resolution. Avoid "high resolution" imaging. At the current state of technology, SNR considerations mandate acquisition of images that are of lower spatial resolution than those used for standard diagnosis. For 2D ASL typical in plane matrices are in the 64x64 to 128x128 range, with corresponding slice thicknesses of 4-6 mm. For 3D ASL isotropic voxels are possible but are often still chosen to be anisotropic due to image acquisition time constraints.
- Signal averaging. To maintain acceptable SNR at reasonable imaging times (4-6 min), multiple signal averages will be required. For 2D techniques, between 30 and 50 signal averages are needed at 3.0T, and even more at 1.5T. For 3D techniques, 2-4 signal averages are required.
- Labeling duration and post labeling delay inversion time (TI). These depend on field strength, ASL method, and expected flow velocities. For brain imaging at 1.5T, labeling durations of 700 ms for PASL and 1500 ms for pCASL with TI values of 1800 are typical. Due to the longer T1 values of blood at 3.0T, slightly longer TI's are required. TI should also be increased whenever slow arterial flows are expected, such as in elderly patients or those with vascular pathology or poor cardiac output. Conversely shorter TI values are recommended for children due to their more rapid circulation times.
- Crusher gradients. Their use is disputed. Although they reduce flow-related artifacts, they require prolongation of the minimum TE, thereby reducing SNR. They also introduce more T2 (T2*) contrast into the ASL image that must be taken into account for quantitative flow measurements. Crusher gradients can also potentially remove important clinical information from the ASL images, such as the presence of delayed or collateral flow.
- Background suppression. Required for segmented 3D imaging methods that use a single excitation per TR. Less effective/efficient for multi-slice 2D methods where they can be considered optional. Background suppression reduce ASL signal slightly (~5%), which should be accounted for if quantitative blood flow measurements are desired.
References
Alsop DC, Detre JA, Gola X, et al. Recommended implementation of arterial spin-labeled
perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med 2015; 73:102-116.
Ferré J-C, Bannier E, Raoult H, et al. Arterial spin labeling (ASL) perfusion: techniques and clinical use. Diagn Interv Radiol 2013; 94:1211-1223
Wong EC. Quantifying CBF with pulsed ASL: technical and pulse sequence factors. J Magn Reson Imaging 2005; 22:727-731.
Ye FQ, Mattay VS, Jezzard P, et al. Correction for vascular artifacts in cerebral blood flow values measured by using arterial spin tagging techniques. Magn Reson Med 1997; 37:226–235. (use of bipolar crusher gradients to suppress ASL signal in large arteries)
Alsop DC, Detre JA, Gola X, et al. Recommended implementation of arterial spin-labeled
perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med 2015; 73:102-116.
Ferré J-C, Bannier E, Raoult H, et al. Arterial spin labeling (ASL) perfusion: techniques and clinical use. Diagn Interv Radiol 2013; 94:1211-1223
Wong EC. Quantifying CBF with pulsed ASL: technical and pulse sequence factors. J Magn Reson Imaging 2005; 22:727-731.
Ye FQ, Mattay VS, Jezzard P, et al. Correction for vascular artifacts in cerebral blood flow values measured by using arterial spin tagging techniques. Magn Reson Med 1997; 37:226–235. (use of bipolar crusher gradients to suppress ASL signal in large arteries)
Related Questions
Can you briefly explain the difference between the various ASL methods? Which is the best?
Can you briefly explain the difference between the various ASL methods? Which is the best?