Using Parallel Imaging
Should parallel imaging acceleration be used in every case?
|
|
Most modern MR systems are built in a parallel architecture, consisting of a body transmit coil and set of local receiver coils that feed into parallel channels for signal amplification and processing. When operated in parallel imaging (PI) mode, information about coil positions and sensitivities can be used to reduce the number of phase-encoding steps and speed up imaging. This is quantified by the PI acceleration factor (R), a number typically between 2 and 6.
The decision to use PI acceleration depends on the spatial and temporal requirements of a particular study, the field strength at which the study is performed, and the object of interest.
The decision to use PI acceleration depends on the spatial and temporal requirements of a particular study, the field strength at which the study is performed, and the object of interest.
The major advantages of PI can be briefly enumerated:
- Significant reduction in image acquisition time. This is inversely related to the acceleration factor (R). If R=2, for example, image acquisition time is cut in half. This time savings can be monetized (time=$/euros/yen), used for additional sequences, or to obtain higher spatial or temporal resolution at the original imaging time.
- Reduction in susceptibility artifacts. Phase-related distortions in the MR signal are lessened by the PI acquisition and reconstruction process. This is especially advantageous in echo-planar sequences.
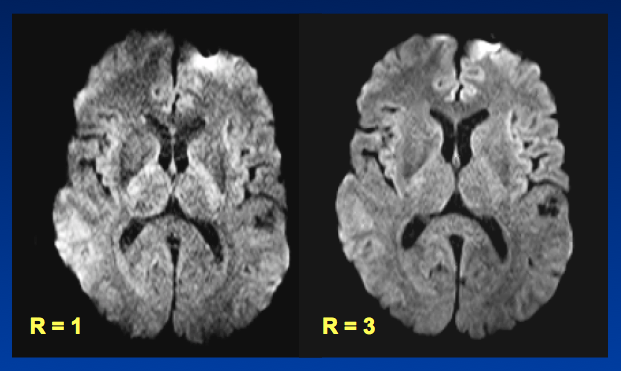
Reduced susceptibility distortions seen on these single-shot DW images using PI
Notwithstanding these benefits, the limitations of PI must be considered:
- Reduction in signal-to-noise ratio (SNR). Even in the absence of motion, all PI techniques extract a significant penalty in terms of SNR. When R=2, image SNR is reduced by √2, or 40%. This disadvantage will be much less of a problem at higher fields (where intrinsic SNR is greater) and in certain anatomic regions (like the brain) that are relatively symmetric and homogeneous.
- Increased PI-specific artifacts. Because PI depends on estimation of coil sensitivities or their harmonic contributions, additional image-processing related artifacts are always present that are non-uniformly distributed. These reconstruction errors increase with the acceleration factor (R) but can be reduced by increasing the number of coil elements.
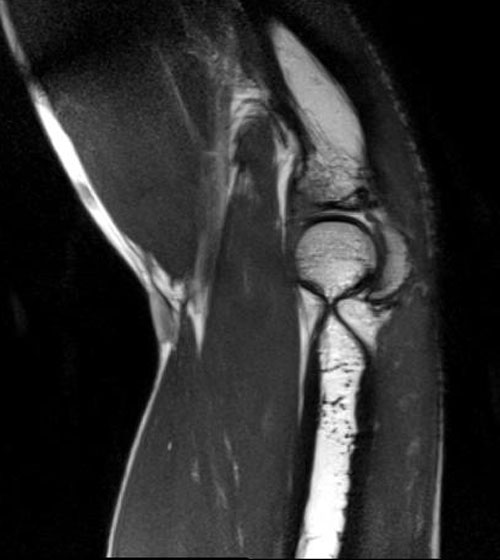
No acceleration (R=1)
|
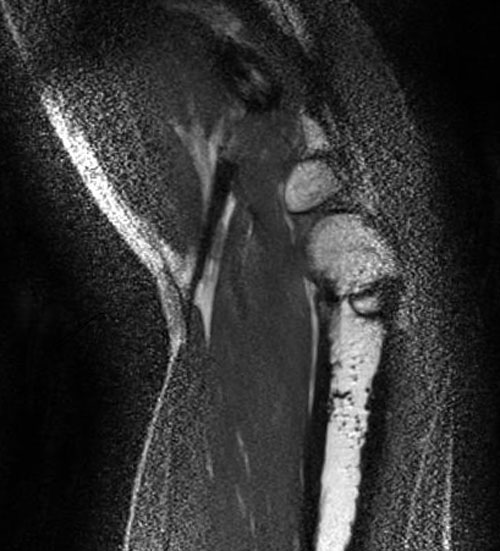
With acceleration (R=4) showing artifacts
|
So, when should you use PI acceleration, and when shouldn't you?
There is no clear "right" or "wrong" answer, and in general the decision must be made by trial and error based on imaging time and image quality. If you can achieve your desired voxel resolution and spatial coverage in a reasonable time frame without using PI, then you are probably better not to use it. At our institution use PI rather sparingly for neuroradiology and musculoskeletal imaging, but use it extensively in chest and abdominal imaging. We also use PI more at 3T than 1.5T. As the techniques and coils continue to evolve, we expect this use to increase in all areas.
References
Deshmane A, Gulani V, Griswold MA, Seiberlich N. Parallel MR imaging. J Magn Reson Imaging 2012;36:55-72. (review)
Glockner JF, Hu HH, Stanley DW, et al. Parallel MR imaging: a user's guide. Radiographics 2005;25:1279-1297.
Larkman DJ, Nunes RG. Parallel magnetic resonance imaging. Phys Med Biol 2007;52:R15-R55 [review]
Yanasak N, Clarke G, Stafford RJ et al. Parallel Imaging in MRI: Technology, applications, and quality control. American Association of Physicists in Medicine. Report No 118. June, 2015.
Deshmane A, Gulani V, Griswold MA, Seiberlich N. Parallel MR imaging. J Magn Reson Imaging 2012;36:55-72. (review)
Glockner JF, Hu HH, Stanley DW, et al. Parallel MR imaging: a user's guide. Radiographics 2005;25:1279-1297.
Larkman DJ, Nunes RG. Parallel magnetic resonance imaging. Phys Med Biol 2007;52:R15-R55 [review]
Yanasak N, Clarke G, Stafford RJ et al. Parallel Imaging in MRI: Technology, applications, and quality control. American Association of Physicists in Medicine. Report No 118. June, 2015.