Intro to Gating/Triggering How are cardiac and respiratory gating performed?
|
|
The oldest and most straightforward way to reduce cardiorespiratory artifacts is to synchronize MR data acquisition to the cardiac or respiratory cycles. This process is known as gating or triggering. The two terms are often used interchangeably.
In the strictest sense, however, triggering is a form of prospective gating where MR data acquisition only begins after detection of a desired physiologic event (an R-wave, peripheral pulse, or specified level of inspiration). Gating, a somewhat broader term than triggering, may be either prospective or retrospective. In retrospective gating, MR data are acquired continuously (not in response to a particular cardiorespiratory "trigger" event). The EKG, pulse, or respiratory level is recorded simultaneously with the MR data. The MR data can then be reordered, grouped, or correlated with phase of the cardiorespiratory cycle. Retrospective gating is the method typically used for cine-cardiac motion studies.
In the strictest sense, however, triggering is a form of prospective gating where MR data acquisition only begins after detection of a desired physiologic event (an R-wave, peripheral pulse, or specified level of inspiration). Gating, a somewhat broader term than triggering, may be either prospective or retrospective. In retrospective gating, MR data are acquired continuously (not in response to a particular cardiorespiratory "trigger" event). The EKG, pulse, or respiratory level is recorded simultaneously with the MR data. The MR data can then be reordered, grouped, or correlated with phase of the cardiorespiratory cycle. Retrospective gating is the method typically used for cine-cardiac motion studies.
Prospective cardiac gating (triggering) acquires data during a specific acquisition window between R-waves.
Retrospective gating collects data continuously then groups and fills k-space according to the phase of the cardiac cycle.
Cardiac Gating
|
Cardiac contraction can be detected by EKG or a peripheral pulse transducer. Some type of EKG-based triggering is mandatory for imaging the heart (and often advisable for imaging of the lower thorax). Peripheral pulse gating cannot be used for heart imaging due to the long and unpredictable delay between cardiac contraction and arrival of the pulse wave to the finger. Peripheral pulse gating is commonly used for peripheral MRA and for cine CSF flow studies, however.
|

Peripheral pulse transducer (photoplethysmograph) from www.biopac.com
|
Cardiac and peripheral pulse gating methods are extremely reliable and widely used, except whenever ventricular arrhythmias are present. The methods require special hardware and software plus several minutes of additional setup time before each scan. Another limitation is that the repetition time (TR) cannot be freely chosen but must be set to a multiple of the beat-to-beat interval.
Respiratory Gating
Imaging of the lower chest and upper abdomen requires some method to freeze diaphragmatic motion. In cooperative patients simple breath-holding may be used in conjunction with rapid imaging techniques such as HASTE or SS-EPI. For uncooperative patients and for studies requiring longer than 20-30 seconds (the average patient breath-hold limit) some sort of respiratory gating technique must be used.

Pneumatic respiratory belt and transducer (from www.biopac.com)
|
Respiratory expansion may be detected by use of a thoracic belt, bellows, or cushion. The belt should be placed around the lower chest for "chest breathers" and around the mid abdomen for "abdominal breathers". Impedance plesmythography devices that measure changes in electrical resistance across the chest with respiration also exist but are not commonly used.
|
Simple respiratory gating requires images to be obtained only during limited portions of the respiratory cycle and incurs a significant time penalty (up to 3x that of an ungated study). Hence prospective respiratory gating is seldom used in its pure form any more. Retrospective compensation methods are still performed, however, using methods that collect or reorder image data according to respiratory phase. In recent years the use of navigator echoes to track diaphragmatic motion has become the most popular method for performing respiratory triggering.
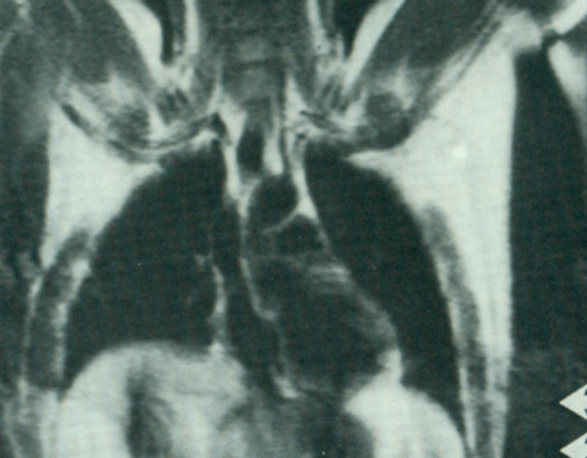
The images below illustrate the effects of simple prospective cardiac and respiratory gating, alone and in combination, to improve MR images of the chest and upper abdomen.
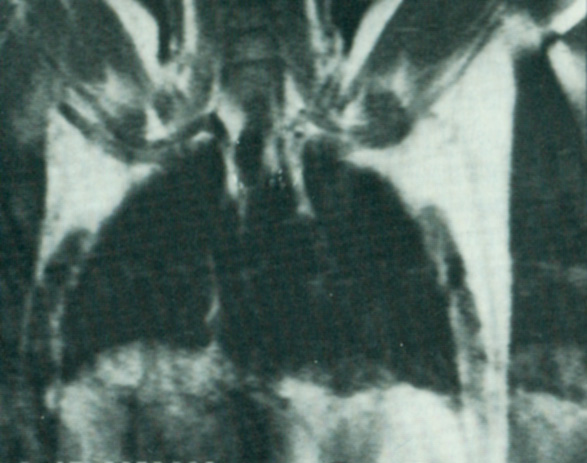
Ungated
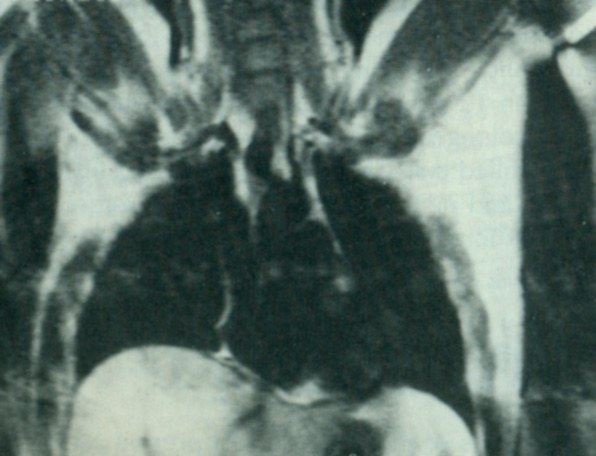
Respiratory gating only
|
Cardiac gating only
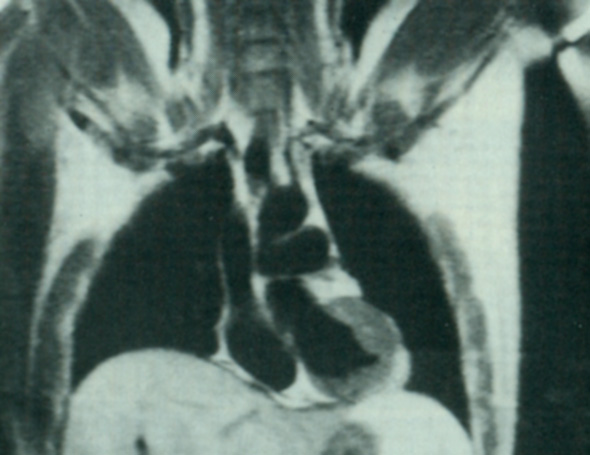
Both cardiac and respiratory gating
|
References
Chia JM, Fischer SE, Wickline SA, Lorenz CH. Performance of QRS detection for cardiac MRI with a novel vectorcardiographic triggering method. J Magn Reson Imaging 2000; 12:678-688.
Ehman RL, McNamara MT, Pallack M, et al. Magnetic resonance imaging with respiratory gating: techniques and advantages. AJR Am J Roentgenol 1984; 143:1175-1182.
Lanzer P, Barta C, Botvinick EH, et al. ECG-synchronized cardiac MR imaging: method and evaluation. Radiology 1985;155:681–686.
Santelli C, Nezafat R, Goddu B, et al. Respiratory bellows revisited for motion compensation: preliminary experience for cardiovascular MR. Magn Reson Med 2011; 65:1097-1102.
Chia JM, Fischer SE, Wickline SA, Lorenz CH. Performance of QRS detection for cardiac MRI with a novel vectorcardiographic triggering method. J Magn Reson Imaging 2000; 12:678-688.
Ehman RL, McNamara MT, Pallack M, et al. Magnetic resonance imaging with respiratory gating: techniques and advantages. AJR Am J Roentgenol 1984; 143:1175-1182.
Lanzer P, Barta C, Botvinick EH, et al. ECG-synchronized cardiac MR imaging: method and evaluation. Radiology 1985;155:681–686.
Santelli C, Nezafat R, Goddu B, et al. Respiratory bellows revisited for motion compensation: preliminary experience for cardiovascular MR. Magn Reson Med 2011; 65:1097-1102.
Related Questions
How do you set the various parameters for a cardiac gated study, such as repetition time (TR), trigger delay, and trigger window?
Is cardiac gating the same as triggering?
What is respiratory compensation? How does this differ from respiratory gating?
How do you set the various parameters for a cardiac gated study, such as repetition time (TR), trigger delay, and trigger window?
Is cardiac gating the same as triggering?
What is respiratory compensation? How does this differ from respiratory gating?