Susceptibility Artifact
What are susceptibility artifacts?
|
|
Susceptibility (χ) is a measure of the extent a substance becomes magnetized when placed in an external magnetic field. Materials that disperse the main field are called diamagnetic. Materials that concentrate the field are called paramagnetic, superparamagnetic, or ferromagnetic, depending on the magnitude of the effect.
Calcium salts (as found in cortical bone) are the most strongly diamagnetic substances in the human body. Nearly all biological tissues (muscle, fat, brain, liver, water) are also diamagnetic, but weakly so. Surprisingly, air is not susceptibility neutral but is slightly paramagnetic due to the presence of molecular oxygen. The presence of metallic ions (Fe, Mn, Gd) in tissues produces weak paramagnetism. Globular microscopic accumulations of iron as seen in ferritin and hemosiderin particles create an even stronger positive susceptibility effect known as superparamagnetism. The most powerful magnetic field susceptibilities occur in solid metal objects containing Fe, Co, or Ni (such as prosthesis, surgical clips, and screws) and is called ferromagnetism.
Calcium salts (as found in cortical bone) are the most strongly diamagnetic substances in the human body. Nearly all biological tissues (muscle, fat, brain, liver, water) are also diamagnetic, but weakly so. Surprisingly, air is not susceptibility neutral but is slightly paramagnetic due to the presence of molecular oxygen. The presence of metallic ions (Fe, Mn, Gd) in tissues produces weak paramagnetism. Globular microscopic accumulations of iron as seen in ferritin and hemosiderin particles create an even stronger positive susceptibility effect known as superparamagnetism. The most powerful magnetic field susceptibilities occur in solid metal objects containing Fe, Co, or Ni (such as prosthesis, surgical clips, and screws) and is called ferromagnetism.
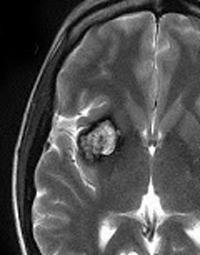
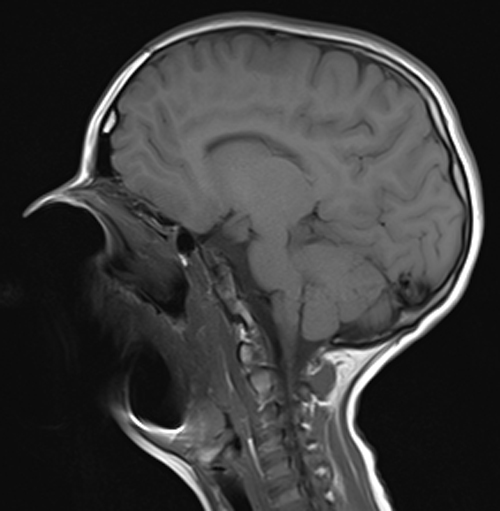
The magnetic field distortions created by susceptibility effects result in variations in precessional frequency across the patient and even within individual voxels. These frequency changes, in turn, produce signal loss from T2*-dephasing and spatial mismapping of the MR signal. The MR imaging characteristics reflect both of these physical mechanisms: geometric distortion with focal areas of signal void and regions of very bright signal resulting from "piling up" signal assigned to the wrong areas. A gallery of various susceptibility artifacts is provided below (click on any picture to enlarge and read caption).
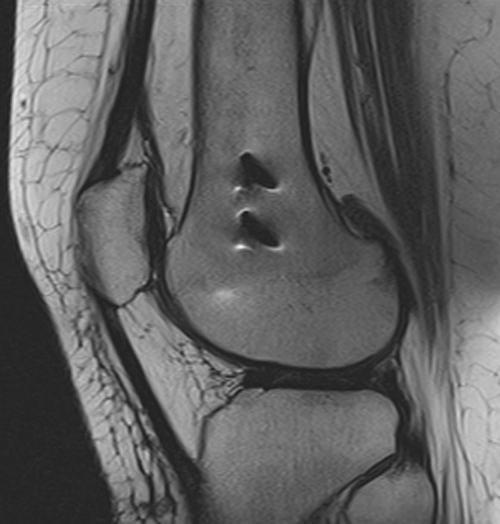


Since ferromagnetic materials have the largest susceptibilities, field distortions and MR artifacts are usually prominent around metal objects and implants. More subtle susceptibility distortions may be seen at natural interfaces (e.g., trabecular bone, paranasal sinuses, skull base, and sella). The shape (diffuse or focal) and intensity (high or low) of the artifact depend on local anatomic relationships, field strength, difference in susceptibilities, echo time (TE) as well as bandwidth (or readout gradient strength and direction) as expressed to the relationship:

Because susceptibility artifacts are worse at high fields, we avoid scanning patients with metal implants at 3.0 T whenever possible. Susceptibility artifacts may be changed in shape, but not eliminated, by altering the directions of frequency- and phase-encoding. They can be minimized by using shorter TE values (less time for dephasing) and by using fast spin-echo instead of gradient-echo sequences. Susceptibility artifacts can also be reduced by increasing gradient strength for a given field-of-view and avoiding narrow bandwidth techniques. Thinner slices also help as do the use of parallel imaging techniques. The more severe metal artifacts may be reduced by specific metal artifact reduction pulse sequences (discussed in the next Q&A).
References
Elster AD. Sellar susceptibility artifacts: theory and implications. AJNR Am J Neuroradiol 1993; 14:129-136. (Explains the physical basis of an artifact at the skull base that can mimic a pituitary adenoma).
Liu H, Martin AJ, Truwit C. Interventional MRI at high field (1.5T): needle artifacts. J Magn Reson Imaging 1998; 8:214-9. (Explains the physical basis of the "blooming ball" artifact at the end of biopsy needles directed parallel to the Bo field).
Port JD, Pomper MG. Quantification and minimization of magnetic susceptibility artifacts on GRE images. J Comput Assist Tomogr 2000;24:958-964.
Schenck JF. The role of magnetic susceptibility in magnetic resonance imaging: MRI magnetic compatibility of the first and second kinds. Med Phys 1996;23:815-850. (Slightly dated, but an excellent and enduring explanation of susceptibility from a pioneer in MRI and first inductee in GE's Genius Hall of Fame).
Elster AD. Sellar susceptibility artifacts: theory and implications. AJNR Am J Neuroradiol 1993; 14:129-136. (Explains the physical basis of an artifact at the skull base that can mimic a pituitary adenoma).
Liu H, Martin AJ, Truwit C. Interventional MRI at high field (1.5T): needle artifacts. J Magn Reson Imaging 1998; 8:214-9. (Explains the physical basis of the "blooming ball" artifact at the end of biopsy needles directed parallel to the Bo field).
Port JD, Pomper MG. Quantification and minimization of magnetic susceptibility artifacts on GRE images. J Comput Assist Tomogr 2000;24:958-964.
Schenck JF. The role of magnetic susceptibility in magnetic resonance imaging: MRI magnetic compatibility of the first and second kinds. Med Phys 1996;23:815-850. (Slightly dated, but an excellent and enduring explanation of susceptibility from a pioneer in MRI and first inductee in GE's Genius Hall of Fame).
Related Questions
What is magnetic susceptibility?
What causes susceptibility?
We recently purchased a metal artifact reduction software for one of our scanners. How does that work?
What is magnetic susceptibility?
What causes susceptibility?
We recently purchased a metal artifact reduction software for one of our scanners. How does that work?