DCE Pulse Sequences
What pulse sequences are used to perform a DCE study?
|
|
|
DCE may be performed on any organ, but is most commonly used for imaging the brain, heart, breast, liver, prostate, and kidney. T1-weighted, 3D-spoiled gradient echo techniques are usually employed, although the exact sequence structure and pulse timing parameters depend on the specific application. Sequences for cardiac perfusion are have some unique features described in a prior Q&A.
|
|
A typical pulse sequence used for brain, breast, or prostate DCE at 1.5 T might be prescribed using the following parameters: Sequence (3D SPGR or FLASH), TR = 4-6 ms, TE = 1-3 ms, flip angle = 10º-15º, and parallel acceleration factor = 2.
The field-of-view, slice thickness, number of slices, and imaging matrix are determined by the application. Breast and prostate DCE studies are often used to characterize small lesions, so for these studies slice thicknesses of ≤ 3 mm and in-plane pixel sizes ≤ 1 mm² are generally required. Brain DCE may not mandate such rigorous spatial resolution, with slice thicknesses as large as 5 mm and pixel sizes up to 50% larger allowed.
The field-of-view, slice thickness, number of slices, and imaging matrix are determined by the application. Breast and prostate DCE studies are often used to characterize small lesions, so for these studies slice thicknesses of ≤ 3 mm and in-plane pixel sizes ≤ 1 mm² are generally required. Brain DCE may not mandate such rigorous spatial resolution, with slice thicknesses as large as 5 mm and pixel sizes up to 50% larger allowed.
Temporal resolution requirements (i.e., the time between phases) and total imaging time vary significantly by organ system and type of image analysis to be performed. A trade-off between spatial and temporal resolution always exists.
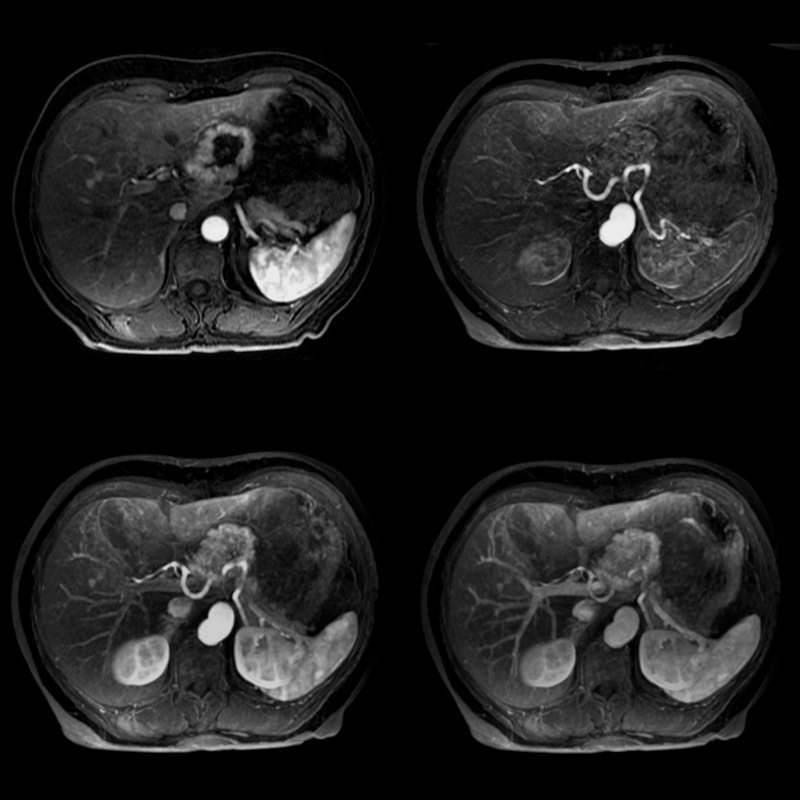 Four phases of a 3D-dynamic contrast enhanced liver
Four phases of a 3D-dynamic contrast enhanced liverstudy using the DISCO technique (Courtesy GE)
For dynamic contrast-enhanced abdominal imaging applications, a 3D spoiled GRE sequence is most commonly employed. Similar sequences offered by the major manufacturers include LAVA (GE), VIBE (Siemens), THRIVE (Philips), and TIGRE (Hitachi). The temporal resolution of these sequences is on the order of 15-20 seconds, which is acceptable for many but not all applications.
More highly accelerated DCE acquisition schemes based on k-space segmentation and random sampling similar to those used in MR angiography (e.g. DISCO) have been used. Parallel imaging methods such as CAIPIRINHA are also becoming popular. Compressed Sensing (CS) methods such as kt-techniques based on sparse sampling also show great promise for DCE applications.
More highly accelerated DCE acquisition schemes based on k-space segmentation and random sampling similar to those used in MR angiography (e.g. DISCO) have been used. Parallel imaging methods such as CAIPIRINHA are also becoming popular. Compressed Sensing (CS) methods such as kt-techniques based on sparse sampling also show great promise for DCE applications.
For breast MR where only semi-quantitative DCE analysis is to be performed, images are typically generated about every 1½−2 minutes and continue for 5−7 minutes. Because prostate neoplasms typically have faster uptake and washout of contrast than breast tumors, the temporal resolution for prostate DCE is more demanding — images must obtained at least every 10 seconds and continue for up to 5 minutes post injection.
Brain DCE imaging is often performed with the intent of generating tissue perfusion parameters based on pharmacokinetic modeling. Such a complete quantitative analysis typically requires an additional pre-contrast T1 mapping protocol that may be either a single Look-Locker type sequence (see related Q&A) or a series of volume acquisitions with different flip angles and echo times. Once T1 mapping has been performed, a spoiled 3D GRE sequence similar to those above is run with temporal resolution in the 5 sec range with collection of data for at least 5 minutes.
References
Buckley DL, Roberts C, Parker GJM, et al. Prostate cancer: evaluation of vascular characteristics with dynamic contrast-enhanced T1-weighted MR imaging — initial experience. Radiology 2004; 233:709-715.
Choi YJ, Kim JK, Kim N, et al. Functional imaging of prostate cancer. RadioGraphics 2007; 27:63-77.
Jahng G-H, Li K-L, Ostergaard l, Calamante F. Perfusion magnetic resonance imaging: a comprehensive update on principles and techniques. Korean J Radiol 2014; 15:554-577. (good recent review).
Larsson HB, Hansen AE, Berg HK, et al. Dynamic contrast-enhanced quantitative perfusion measurement of the brain using T1-weighted MRI at 3T. J Magn Resona Imaging 2008; 27:754-762.
Saranathan M, Rettmann DW, Hargreaves BA, et al. DIfferential Subsampling with Cartesian Ordering (DISCO); a high spatio-temporal resolution Dixon imaging sequence for multiphasic contrast enhanced abdominal imaging. J Magn Reson Imaging 2012; 35:1484-92.
Sourbron S, Ingrisch M, Siefert A, et al. Quantification of cerebral blood flow, cerebral blood volume, and blood-brain-barrier leakage with DCE-MRI. Magn Reson Med 2009; 62:205-217.
Tofts PS. T1-weighted DCE imaging concepts: modelling, acquisition and analysis. MAGNETOM Flash 2010; 3:30-35.
Verma S, Turkbey B, Muradyan N, et al. Overview of dynamic contrast-enhanced MRI in prostate cancer diagnosis and management. AJR Am J Roentgenol 2012; 198:1277-1288. (Prostate DCE requires high temporal resolution, with images acquired every 5-10 sec for several minutes).
Buckley DL, Roberts C, Parker GJM, et al. Prostate cancer: evaluation of vascular characteristics with dynamic contrast-enhanced T1-weighted MR imaging — initial experience. Radiology 2004; 233:709-715.
Choi YJ, Kim JK, Kim N, et al. Functional imaging of prostate cancer. RadioGraphics 2007; 27:63-77.
Jahng G-H, Li K-L, Ostergaard l, Calamante F. Perfusion magnetic resonance imaging: a comprehensive update on principles and techniques. Korean J Radiol 2014; 15:554-577. (good recent review).
Larsson HB, Hansen AE, Berg HK, et al. Dynamic contrast-enhanced quantitative perfusion measurement of the brain using T1-weighted MRI at 3T. J Magn Resona Imaging 2008; 27:754-762.
Saranathan M, Rettmann DW, Hargreaves BA, et al. DIfferential Subsampling with Cartesian Ordering (DISCO); a high spatio-temporal resolution Dixon imaging sequence for multiphasic contrast enhanced abdominal imaging. J Magn Reson Imaging 2012; 35:1484-92.
Sourbron S, Ingrisch M, Siefert A, et al. Quantification of cerebral blood flow, cerebral blood volume, and blood-brain-barrier leakage with DCE-MRI. Magn Reson Med 2009; 62:205-217.
Tofts PS. T1-weighted DCE imaging concepts: modelling, acquisition and analysis. MAGNETOM Flash 2010; 3:30-35.
Verma S, Turkbey B, Muradyan N, et al. Overview of dynamic contrast-enhanced MRI in prostate cancer diagnosis and management. AJR Am J Roentgenol 2012; 198:1277-1288. (Prostate DCE requires high temporal resolution, with images acquired every 5-10 sec for several minutes).
Related Questions
How is cardiac T1 mapping performed? When is it useful?
Does breast DCE require any special techniques?
What is CAIPIRINHA? Isn't it some sort of a drink?
How is cardiac T1 mapping performed? When is it useful?
Does breast DCE require any special techniques?
What is CAIPIRINHA? Isn't it some sort of a drink?