MR Safety: Spinal Cord Stimulators
Can patients with spinal cord stimulators undergo MRI?
|
|
|
Spinal cord stimulation (SCS) is indicated for the management of chronic intractable pain of the back, trunk, or extremities. The typical system consists of a implanted pulse generator (IPG) located subcutaneously in the flank or lower abdomen connected by insulated lead(s) to a cylindrical or paddle-shaped electrode array placed in the posterior epidural space of the mid-to-lower thoracic spine. Permanent implantation usually follows a trial period wherein smaller cylindrical epidural test electrodes are placed in the epidural space percutaneously, with wires protruding out through the skin where they are attached to an external pulse generator. If the trial is successful at reducing pain, then a full system with a permanent pulse generator is implanted. If a paddle array is chosen, a laminectomy is required for placement.
|
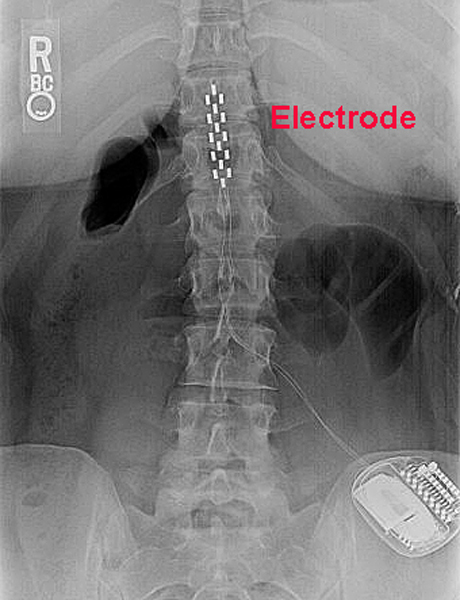
Typical configuration of an "MR Conditional" SCS with paddle electrode array
|
During the 2000s about a dozen companies sold and manufactured SCS systems worldwide, including the "big three" (Boston Scientific, Abbott/St. Jude, Medtronic). Most of the early models of these devices were considered MR Unsafe primarily due to the theoretical risk of spinal cord injury from heating of the the electrode tip by RF-induced currents (the so-called antenna effect). Additional concerns included damage to the IPG or its battery, opening of the magnetic reed switch, or resetting of IPG programming.
Although more recent SCS systems are designed to be MR Conditional, a substantial number of MR Unsafe legacy devices may still be encountered in clinical practice. A partial list includes: the Boston Scientific Precision® and Precision Novi®; the Medtronic X-trel®, I-trel®, and early Matrix® systems; the Abbott/St. Jude Eon®, Genesis®, Axium®, and Renew®. Notwithstanding legal and risk management issues, it may be possible (similar to the experience with legacy pacemakers) to perform low SAR MR imaging in selected patients if clinically necessary.
A new generation of MR Conditional SCSs (such as the Evoke® (Saluda Medical)) have resulted from several technical advances: electromagnetic interference circuit protection filtering (“filtered feed-through"); reduction in ferrous material in the IPG; replacement of magnetic reed switches by Hall effect sensors; and lead design changes with internal spiral conductors. The precise conditions that must be followed for safe MR Scanning of SCS systems vary somewhat among the models and manufacturers.
What are the Conditions?
- Device identification. The exact model/serial numbers from the various components of the SCS system, including the IPG, leads, and extensions (if present) must be established with certainty. This can be done by reviewing operative notes from the medical record or the patient's information card.
- Determine location of components. Verify (by x-ray if necessary) that the IPG has been implanted subcutaneously in the pelvis/flank. Insure that the wires are connected to the IPG without breaks and there are no abandoned leads or electrodes.
- Pre-MRI evaluation/interrogation of the DBS system. The IPG battery should be fully charged and lead impedances should measure within expected values. The IPG should be turned off or placed in "MRI Mode" if available.
- MRI Equipment and Protocols. These conditions will vary significantly between manufacturers and SCS models. All current MR-conditional SCS devices are restricted to ¹H imaging in horizontal bore cylindrical magnets operating at 1.5 or 3.0T. Only the supine or prone patient positions are allowed. Limits for maximum spatial gradient, gradient slew rate, total imaging time, and RF power dissipation measured by average SAR or maximum B1+RMS must be followed explicitly. For several models there are restrictions on the use of transmit body coils and power deposition limits dependent on the location of magnet isocenter.
- Before, During, and After MRI. The patient must be in a cognitive state able to provide immediate feedback concerning any problems during the examination. Visual and auditory monitoring should be continuously performed during the scan. After the exam, MRI-mode should be turned off and settings returned to pre-MRI values.
References
De Andres J, Valía JC, Cerda‐Olmedo G et al. Magnetic resonance imaging in patients with spinal neurostimulation systems. Anesthesiology 2007; 106:779-786. (It may be possible to perform MRI in selected patients with "MR Unsafe" legacy SCSs if care is taken).
Moens M, Droogmans S, Spapen H, et al. Feasibility of cerebral magnetic resonance imaging in patients with externalized spinal cord stimulator. Clin Neurol Neurosurg 2012; 114:135-141.
Rubino S, Adepoju A, Kumar V, et al. MRI conditionality in patients with spinal cord stimulation devices. Sterotact Funct Neurosurg 2016; 94:254-258
Shellock FG, Audet-Griffin AJ. Evaluation of magnetic resonance imaging issues for a wirelessly powered lead used for epidural, spinal cord stimulation. Neuromodulation 2014;17:334–339. (testing of the Freedom-4 externally powered SCS).
Tronnier VM, Staubert A, Hähnel S, Sarem-Alsani A. Magnetic resonance imaging with implanted neurostimulators: An in vitro and in vivo study. Neurosurgery 1999; 44:118-126.
De Andres J, Valía JC, Cerda‐Olmedo G et al. Magnetic resonance imaging in patients with spinal neurostimulation systems. Anesthesiology 2007; 106:779-786. (It may be possible to perform MRI in selected patients with "MR Unsafe" legacy SCSs if care is taken).
Moens M, Droogmans S, Spapen H, et al. Feasibility of cerebral magnetic resonance imaging in patients with externalized spinal cord stimulator. Clin Neurol Neurosurg 2012; 114:135-141.
Rubino S, Adepoju A, Kumar V, et al. MRI conditionality in patients with spinal cord stimulation devices. Sterotact Funct Neurosurg 2016; 94:254-258
Shellock FG, Audet-Griffin AJ. Evaluation of magnetic resonance imaging issues for a wirelessly powered lead used for epidural, spinal cord stimulation. Neuromodulation 2014;17:334–339. (testing of the Freedom-4 externally powered SCS).
Tronnier VM, Staubert A, Hähnel S, Sarem-Alsani A. Magnetic resonance imaging with implanted neurostimulators: An in vitro and in vivo study. Neurosurgery 1999; 44:118-126.
Related Questions
Can patients with deep brain stimulators be scanned?
Can patients with deep brain stimulators be scanned?