MR Safety: Epicardial CIEDsWhat about epicardial CIED's and their abandoned leads?
|
|
|
Permanently Implanted Epicardial CIEDs
These devices are quite uncommon and implanted by surgeons. They are used principally in infants and children with complex congenital heart disease (where endovascular access may be difficult to obtain) and in adults with endocarditis and/or previous hardware infections. To my knowledge no specific research about the MR safety of such devices exists. If encountered, I believe they should be handled as you would any other non-Conditional CIEDs as described in the dedicated Q&A on this topic. |
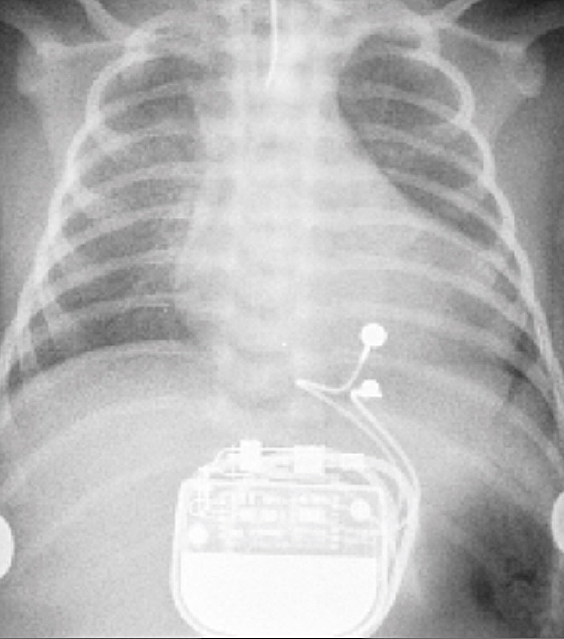
Permanent epicardial pacemaker in a child with congenital heart disease
From Costa et al under CC-BY |
Temporary Epicardial Pacemakers
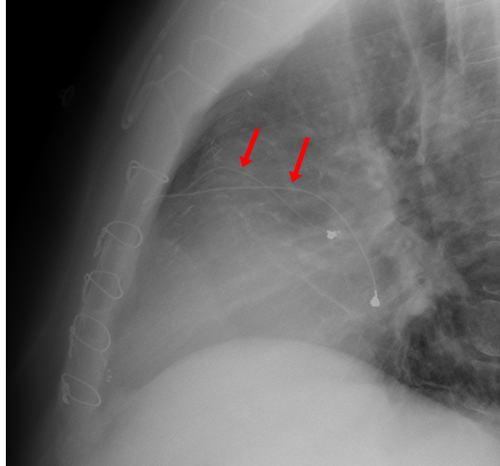 Epicardial pacing wires
Epicardial pacing wires
Temporary epicardial pacemakers and wires are commonly placed after open heart surgery to treat possible arrhythmias that might develop in the postoperative period. The leads are passed through the mediastinum and subcutaneously to protrude through the skin where they are connected to an external pulse generator. After the patient proves rhythmically stable (typically 2 - 14 days postoperatively), the external unit is removed and the wires are manually pulled from the chest. Although usually extracted successfully, it is not rare for the wires to break off under the skin and be retained. Because of their short length, absence of large loops, and subcutaneous location, such retained epicardial pacing wire fragments are not considered a contraindication to MR imaging.
In the rare situation where the wires have not been removed or broken off but are still intact and protruding though the skin, we have on rare occasions scanned such patients safely. (This assumes that the patient is not dependent on the extracorporeal pacemaker). With the external pulse generator removed, the protruding wires should be lifted and straightened to lie parallel to the long axis of the patient. The wires should be separated from each other and padded so they do not touch the patient's skin (to reduce risk of cutaneous burns).
In the rare situation where the wires have not been removed or broken off but are still intact and protruding though the skin, we have on rare occasions scanned such patients safely. (This assumes that the patient is not dependent on the extracorporeal pacemaker). With the external pulse generator removed, the protruding wires should be lifted and straightened to lie parallel to the long axis of the patient. The wires should be separated from each other and padded so they do not touch the patient's skin (to reduce risk of cutaneous burns).
References
Costa R, da Silva K, Filho MM, Carrillo R. Minimally invasive epicardial pacemaker implantation in neonates with congenital heart block. Arq Bras Cardiol 2017; 109:331-339.
Hartnell GG, Spence L, Hughes LA, et al. Safety of MR imaging in patients who have retained metallic materials after cardiac surgery. AJR Am J Roentgenol 1997; 168: 1157–1159.
Costa R, da Silva K, Filho MM, Carrillo R. Minimally invasive epicardial pacemaker implantation in neonates with congenital heart block. Arq Bras Cardiol 2017; 109:331-339.
Hartnell GG, Spence L, Hughes LA, et al. Safety of MR imaging in patients who have retained metallic materials after cardiac surgery. AJR Am J Roentgenol 1997; 168: 1157–1159.
Related Questions
How strictly must one follow the MR conditions for CIEDs if you feel a patient needs an MRI scan? Which can be violated with the least risk?
How strictly must one follow the MR conditions for CIEDs if you feel a patient needs an MRI scan? Which can be violated with the least risk?