Advanced DSC ProcessingHow is the arterial input function used to extract more quantitative flow information from the DSC data?
|
|
Conversion of raw DSC imaging data into quantitative blood flow measurements takes place in three steps:
- Translation of tissue MR signal s(t) into gadolinium concentration c(t);
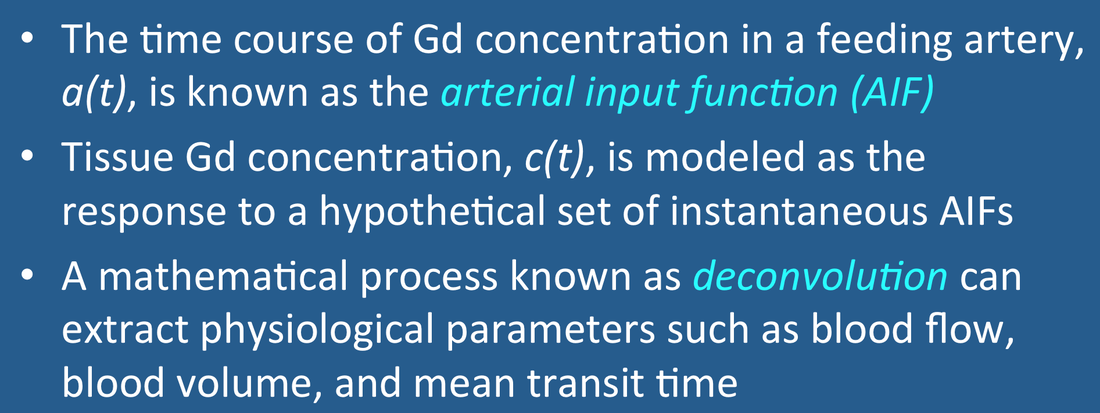
- Selection of an appropriate arterial input function a(t); and
- Mathematical modeling and computation.
|
The first two steps have been described in prior Q&As. This section addresses mathematical methods to quantify blood flow knowing only c(t) and a(t). The analysis comes from from linear systems theory and requires several important assumptions:
|
The reader will immediately recognize how easily this simple model may fail in practice. For example, a brain tumor accumulating gadolinium contrast through a leaky blood-brain-barrier would not meet assumption #2. |
Blood volume (V) is the first and easiest parameter to extract. Assuming no leakage or recirculation effects, V is proportional to the area under the tissue concentration curve c(t) during the first pass of contrast. Theoretically this relationship can be made quantitative by dividing by the gadolinium concentration a voxel containing only blood. Typically such a reference voxel is chosen to lie within a feeding artery, and the arterial input function curve, a(t), is convenient to use. (A voxel from a large vein can also be chosen, a common practice in CT perfusion studies). In mathematical form

Blood flow (F) is the next parameter to be calculated, but the process for doing so is somewhat "convoluted". (Please forgive the old physics pun). Understanding the method requires a brief introduction to linear systems theory.
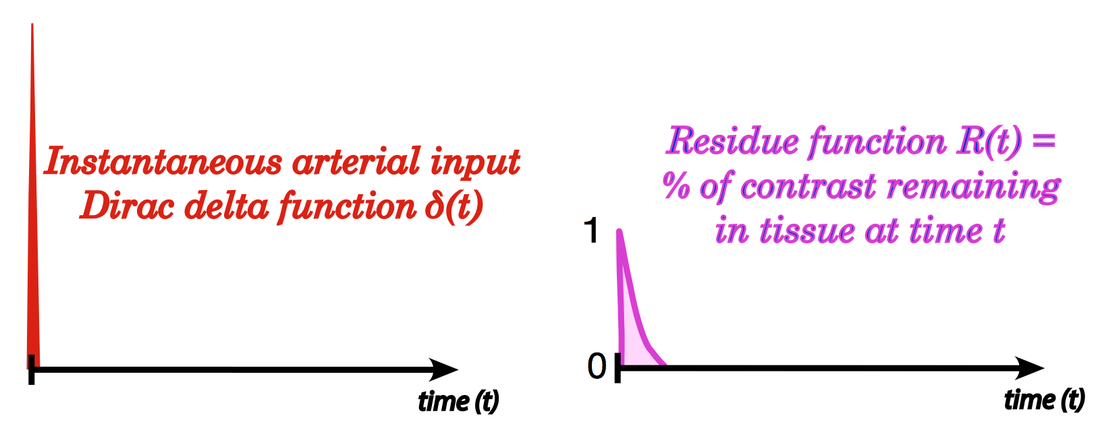
A linear system (e.g., the tissue capillary bed) can be analyzed by considering its response to a hypothetical infinitely high intensity, infinitely short duration impulse called the Dirac delta function δ(t). For our system δ(t) could be viewed as the instantaneous injection of a bolus of contrast particles into the tissue through an arterial port at time t=0. After injection, some of these particles will find relatively direct pathways to the venous port; others will choose more circuitous routes and take longer to traverse the capillary bed. This results in a dispersion of the injected contrast bolus within tissue and a range of particle transit times.
The fraction of injected contrast particles remaining in the tissue at time t after such an impulse injection is known as the residue, described by the dimensionless function R(t). Immediately after injection (before any particles have left the system) R(t) is at its maximum with value R(0) = 1. As particles flow out of the system, R(t) decreases, eventually reaching final value R(∞) = 0 when no contrast remains in the tissue.
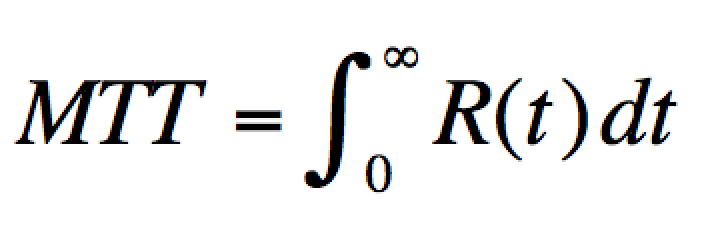
The width of the residue function reflects the distribution of particle transit times through a tissue. Tissues with rapid transit times have sharp, narrow residue curves, while tissues with prolonged transit times have wide ones. The area under the residue function reflects the average time a particle spends transitioning through the tissue vascular bed, an important physiological parameter known as the mean transit time (MTT). In mathematical form
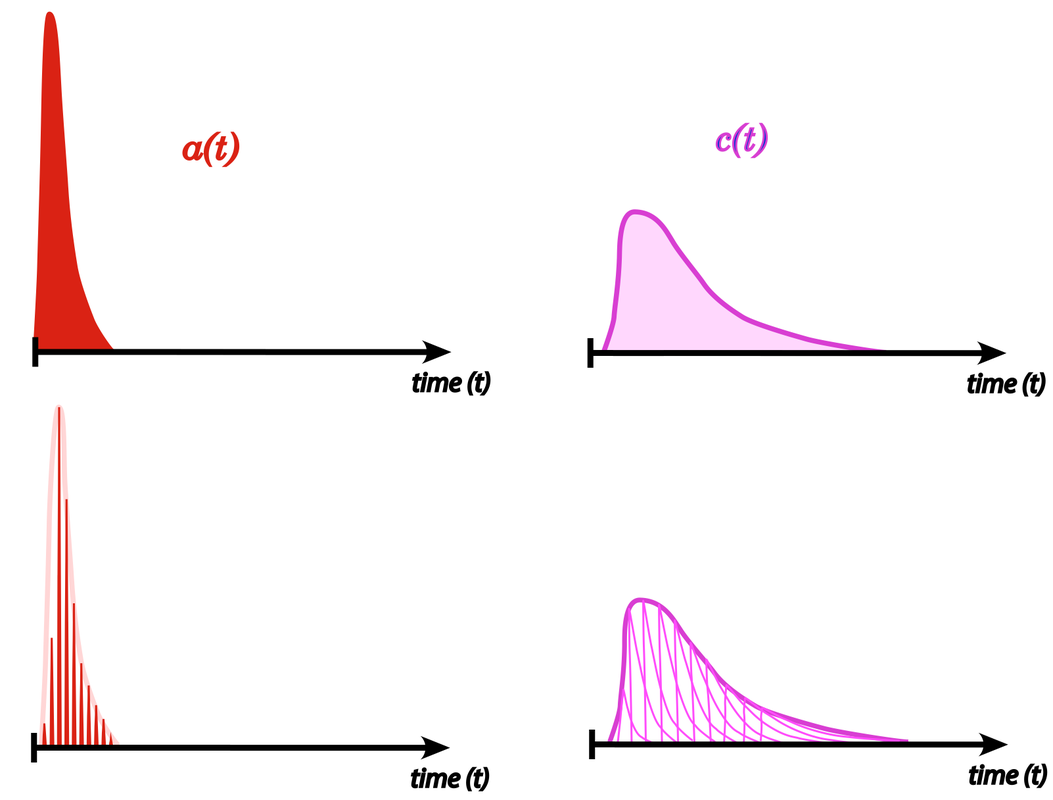
Upper figures: a real-life arterial input function (AIF) with corresponding resultant tissue concentration curve c(t)
Lower figures: modeling the tissue response by a set of Dirac delta functions |
In real life it is impossible to deliver an
arterial bolus of contrast to tissue instantaneously. The arterial input function, a(t), is thus always dispersed in time as shown in the figure. This broad arterial input, however, can be represented as a set of Dirac delta functions at different time delays (τ), each producing an independent response. The mathematical operation of scaling and summing these individual impulse responses to generate the tissue contrast concentration curve c(t) is known as convolution. In mathematical notation
|

where F is blood flow and the "circle/x" symbol is the convolution operator. The convolution process sums together ("integrates") the individual arterial inputs weighted ("multiplied") by the residue function at various time delays (τ) after injection. To account for the fact that gadolinium contrast distributes only in the extracellular space of blood vessels, some versions of this equation contain a constant factor (ρ/h) preceding F, where ρ is the tissue density in g/mL and h is a fraction accounting for the difference in hematocrit between capillaries and larger vessels.
In a DSC perfusion experiment we measure a(t) and c(t) directly, but do not know either the blood flow (F) nor the residue function, R(t). Because there are more unknowns than knowns in this equation, a unique solution does not exist. Nevertheless, various mathematical techniques can extract reasonable estimates for these parameters, especially blood flow (F).
Three general strategies for performing mathematical deconvolution exist. The most common method converts the equation into matrix form and perform iterative calculations with a procedure known as singular value decomposition (SVD). A second approach, less widely used, is called "parametric", because it assumes a predetermined shape for the residue function such as a decaying exponential. Other deconvolution techniques involve Fourier transformation or stochastic estimation.
The end result of all the deconvolution methods is a quantitative estimate for blood flow (F). Since blood volume (V) has already been calculated, the final step is to compute the mean transit time (MTT) on a voxel-by-voxel basis using the central volume theorem (MTT = V/F).
It should be noted that significantly different results may be obtained depending on the choice of the AIF as well as which commercial software product for calculation is used. Even software claiming to use identical methods may give different results when applied to the same raw data. Caution is advised in relying too heavily on the absolute numbers obtained from such quantitative methods.
The concept of (de)convolution is admittedly confusing for those without a strong mathematical background, but my colleague Josh Shimony makes it quite understandable in this vimeo video beginning at about minute 33:00. The whole video is a great introduction to both DSC and ASL, so if you have an extra hour I suggest you watch it in its entirety.
Josh Shimony: MRI Perfusion from NRG on Vimeo.
References
Boxerman JL, Rosen BR, Weisskoff RM. Signal-to-noise analysis of cerebral blood volume maps from dynamic NMR imaging studies. J Magn Reson Imaging 1997; 7:528-37.
Calamante F, Christensen S, Desmond PM, et al. The physiological significance of the time-to-maximum (Tmax) parameter in perfusion MRI. Stroke 2010; 41:1169-1174. (See Advanced Discussion tab for why I don't favor this parameter in practice.)
Fieselmann A, Kowarschik M, Ganguly A, et al. Deconvolution-based CT and MR brain perfusion measurement: theoretical model revisited and practical implementation details. Int J Biomed Imag 2011; doi:10/1155/2011/467563
Orsingher L, Piccinini S, Crisi G. Differences in dynamic susceptibility contrast MR perfusion maps generated by different methods implemented in commercial software. J Comput Assist Tomogr 2014; 38:647-654. (different software gives different results, even when methods are said to be the same!)
Østergaard L, Weisskoff RM, Chesler DA, et al. High resolution measurement of cerebral blood flow using intravascular tracer bolus passages. Part I. Mathematical approach and statistical analysis. Magn Reson Med 1996; 36:715-725. (good description of deconvolution techniques including Fourier and SVD).
Zaharchuk G. Theoretical basis of hemodynamic MR imaging techniques to measure cerebral blood volume, cerebral blood flow, and permeability. AJNR Am J Neuroradiol 2007; 28:1850-8.
Boxerman JL, Rosen BR, Weisskoff RM. Signal-to-noise analysis of cerebral blood volume maps from dynamic NMR imaging studies. J Magn Reson Imaging 1997; 7:528-37.
Calamante F, Christensen S, Desmond PM, et al. The physiological significance of the time-to-maximum (Tmax) parameter in perfusion MRI. Stroke 2010; 41:1169-1174. (See Advanced Discussion tab for why I don't favor this parameter in practice.)
Fieselmann A, Kowarschik M, Ganguly A, et al. Deconvolution-based CT and MR brain perfusion measurement: theoretical model revisited and practical implementation details. Int J Biomed Imag 2011; doi:10/1155/2011/467563
Orsingher L, Piccinini S, Crisi G. Differences in dynamic susceptibility contrast MR perfusion maps generated by different methods implemented in commercial software. J Comput Assist Tomogr 2014; 38:647-654. (different software gives different results, even when methods are said to be the same!)
Østergaard L, Weisskoff RM, Chesler DA, et al. High resolution measurement of cerebral blood flow using intravascular tracer bolus passages. Part I. Mathematical approach and statistical analysis. Magn Reson Med 1996; 36:715-725. (good description of deconvolution techniques including Fourier and SVD).
Zaharchuk G. Theoretical basis of hemodynamic MR imaging techniques to measure cerebral blood volume, cerebral blood flow, and permeability. AJNR Am J Neuroradiol 2007; 28:1850-8.
Related Questions
What is the arterial input function (AIF) and why do you need to measure it?
How are parameters like BF, BV, and MTT defined and used in perfusion imaging?
What is the arterial input function (AIF) and why do you need to measure it?
How are parameters like BF, BV, and MTT defined and used in perfusion imaging?