SSFP MRA
What is SSFP MRA and how does it work? When would I want to use this technique?
|
|
Balanced steady-state free precession (b-SSFP) techniques based on TrueFISP (FIESTA) sequences are widely used for noncontrast MRA of the chest, abdomen, and pelvis. TrueFISP/FIESTA are rapid gradient-echo sequences in which the free induction decay (FID) and spin/stimulated echo components are made to coincide in the middle of the TR interval. As described in a prior Q&A, this structure allows a coherent transverse steady state to become established, whose maximum signal intensity depends on the ratio T2/T1 of the tissue being imaged.
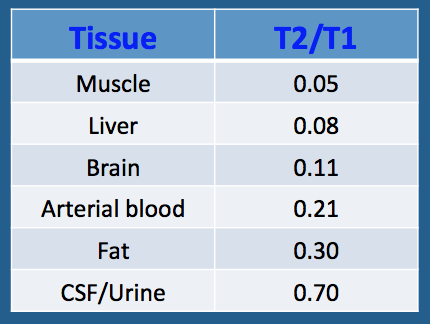 Approximate T2/T1 ratios at 1.5T
Approximate T2/T1 ratios at 1.5T
b-SSFP MRA exploits the differences between the relatively high T2/T1 ratio of blood compared to most other tissues. As seen in the table left, most solid tissues have low T2/T1 ratios, on the order of 0.05−0.10 at 1.5T. Blood, fat, and pure fluids have much higher T2/T1 values and therefore appear intrinsically bright on SSFP sequences.
An important concept is that image contrast in b-SSFP MRA sequences derives principally from the relaxation properties of blood itself. The appearance of vessels is relatively insensitive to a wide range of blood velocities, direction of flow, or phase of the cardiac cycle.
Because of their gradient symmetry, b-SSFP sequences are intrinsically flow-compensated in all three directions. Some signal loss on SSFP MRA does occur with high degrees of turbulence or rapid jets across stenotic lesions, but these phenomena can be useful to identify and assess the significance of such abnormalities.
Because both fat and fluids also have high T2/T1 ratios, their presence next to blood vessels may compromise the quality of a b-SSFP MRA study. In fact, the b-SSFP method is not suitable for intracranial MRA where vessels normally reside in a bath of high-signal cerebrospinal fluid (CSF). Small vessels such as the coronary, renal, or mesenteric arteries may also be obscured by high signal from the nearby fat in which they are embedded. Commonly an adjuvant fat suppression method is used when performing b-SSFP MRA of these vessels.
An important concept is that image contrast in b-SSFP MRA sequences derives principally from the relaxation properties of blood itself. The appearance of vessels is relatively insensitive to a wide range of blood velocities, direction of flow, or phase of the cardiac cycle.
Because of their gradient symmetry, b-SSFP sequences are intrinsically flow-compensated in all three directions. Some signal loss on SSFP MRA does occur with high degrees of turbulence or rapid jets across stenotic lesions, but these phenomena can be useful to identify and assess the significance of such abnormalities.
Because both fat and fluids also have high T2/T1 ratios, their presence next to blood vessels may compromise the quality of a b-SSFP MRA study. In fact, the b-SSFP method is not suitable for intracranial MRA where vessels normally reside in a bath of high-signal cerebrospinal fluid (CSF). Small vessels such as the coronary, renal, or mesenteric arteries may also be obscured by high signal from the nearby fat in which they are embedded. Commonly an adjuvant fat suppression method is used when performing b-SSFP MRA of these vessels.

|
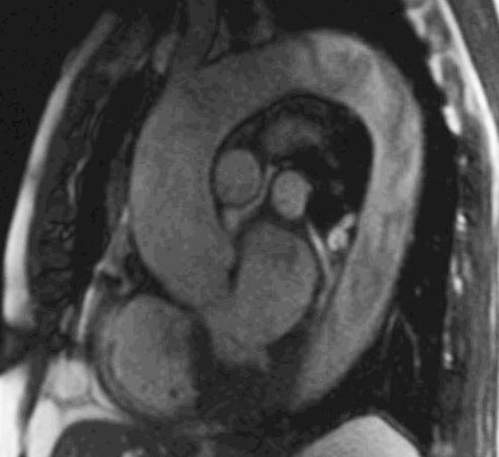
Left: SSFP (TrueFISP) thoracic aortogram
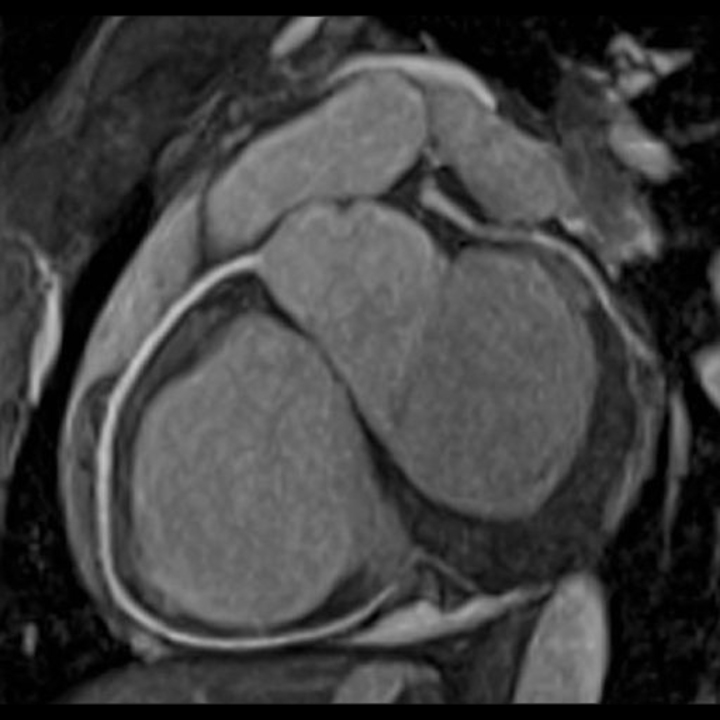
Above: Gated SSFP (TrueFISP) coronary artery image with fat suppression |
Intrinsic high signal of adjacent veins may not be a problem for b-SSFP imaging of large structures like the cardiac chambers or the thoracic aorta, but can create problems in visualizing smaller vessels such as the renal arteries where veins are in close proximity. A variety of inversion recovery-based saturation methods are commonly used to suppress venous inflow, enhance arterial inflow, or both. These will be described in subsequent Q&A's.
Cardiac-gated, cine b-SSFP-MRA is the principal technique used for functional cardiac imaging to assess chamber size, wall motion abnormalities, regurgitation, shunting, and cardiac output. These methods will be described in detail in the Cardiac MR Tab following the current one.
|
The major limitation of balanced SSFP-MRA is its sensitivity to field inhomogeneities, with the occurrence of zebra-stripe (Moiré) artifacts especially near the edges of the image. Anatomic distortions may occur at air-tissue interfaces or in the presence of nearby metallic foreign bodies, especially surgical clips and stents. Although additional localized shimming prior to imaging is may reduce these artifacts, they often cannot be eliminated.
|

b-SSFP zebra-stripe phase artifacts (arrow)
|
Flow artifacts in descending aorta on b-SSFP
|
SSFP techniques also suffer due to signal contributions from flowing spins that have already exited the imaging slice. Gradient activity in SSFP in not confined to the region of the RF-excitations. The balanced nature of these gradients permits “out-of-slice” transverse magnetization to contribute to the total SSFP signal. This results in broadening of slice thickness for flowing spins, frequency dependence of flow-related enhancement, and increased flow-related artifacts. |
References
Miyazaki M, Lee VS. Nonenhanced MR angiography. Radiology 2008;248:20-43.
Scheffler K, Lehnhardt S. Principles and applications of balanced SSFP techniques. Eur Radiol 2003; 13: 2409-2418.
Miyazaki M, Lee VS. Nonenhanced MR angiography. Radiology 2008;248:20-43.
Scheffler K, Lehnhardt S. Principles and applications of balanced SSFP techniques. Eur Radiol 2003; 13: 2409-2418.
Related Questions
What is True FISP, and why is it "truer" than regular FISP?
How do inflow-enhanced SSFP MRA sequences work? Where do you place the saturation bands?
What is True FISP, and why is it "truer" than regular FISP?
How do inflow-enhanced SSFP MRA sequences work? Where do you place the saturation bands?